{"title":"Establishment of a swine experimental model of non-occlusive mesenteric ischemia: Combining induced hemorrhagic shock and vasopressor administration","authors":"Yasutaka Tanaka, Yosuke Matsumura, Makoto Aoki, Yosuke Hayashi, Yoshimitsu Izawa, Kazuhiro Endo, Takashi Mato","doi":"10.1002/ams2.982","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Non-occlusive mesenteric ischemia (NOMI) is associated with high mortality rates, but definitive treatments have not yet been established. Although experimental animal models are worthwhile, reproducible models that reflect the pathophysiology of NOMI have not been developed.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We combined risk factors for NOMI, comprising hemorrhagic shock, systemic vasopressor infusion, and local vasopressor infusion from the superior mesenteric artery (SMA) in swine under maintained anesthesia. Experiment 1 involved full-intensity (40%) phlebotomy and systemic vasopressor (norepinephrine and epinephrine). Experiment 2 involved full-intensity (40%) phlebotomy, systemic norepinephrine, and local vasopressor infusion into the SMA. Experiment 3 involved moderate (27%) phlebotomy, systemic norepinephrine infusion, and local epinephrine infusion. We evaluated serum lactate levels, intestinal serosa color, computed tomography (CT) angiography, and pathological findings.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>After inducing hemorrhage, systemic vasopressor alone and in combination with local vasopressin or norepinephrine infusion did not induce ischemic color changes in the intestine. The combination of systemic norepinephrine and local epinephrine (0.5 μg/kg/min) after moderate (27% blood loss) hemorrhage induced gross color change, pathological destruction, and elevation of serum lactate. Patent flow in the SMA was confirmed on CT angiography.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>We established a swine NOMI model with systemic norepinephrine infusion and local epinephrine with moderate hemorrhagic shock.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11263749/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.982","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Aim
Non-occlusive mesenteric ischemia (NOMI) is associated with high mortality rates, but definitive treatments have not yet been established. Although experimental animal models are worthwhile, reproducible models that reflect the pathophysiology of NOMI have not been developed.
Methods
We combined risk factors for NOMI, comprising hemorrhagic shock, systemic vasopressor infusion, and local vasopressor infusion from the superior mesenteric artery (SMA) in swine under maintained anesthesia. Experiment 1 involved full-intensity (40%) phlebotomy and systemic vasopressor (norepinephrine and epinephrine). Experiment 2 involved full-intensity (40%) phlebotomy, systemic norepinephrine, and local vasopressor infusion into the SMA. Experiment 3 involved moderate (27%) phlebotomy, systemic norepinephrine infusion, and local epinephrine infusion. We evaluated serum lactate levels, intestinal serosa color, computed tomography (CT) angiography, and pathological findings.
Results
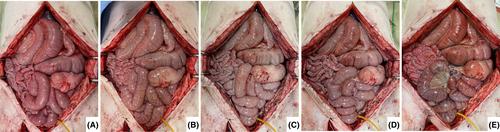
After inducing hemorrhage, systemic vasopressor alone and in combination with local vasopressin or norepinephrine infusion did not induce ischemic color changes in the intestine. The combination of systemic norepinephrine and local epinephrine (0.5 μg/kg/min) after moderate (27% blood loss) hemorrhage induced gross color change, pathological destruction, and elevation of serum lactate. Patent flow in the SMA was confirmed on CT angiography.
Conclusion
We established a swine NOMI model with systemic norepinephrine infusion and local epinephrine with moderate hemorrhagic shock.
目的:非闭塞性肠系膜缺血(NOMI)与高死亡率有关,但目前尚未确立明确的治疗方法。尽管实验动物模型很有价值,但反映 NOMI 病理生理学的可重复模型尚未开发出来:方法:我们结合了NOMI的风险因素,包括失血性休克、全身血管加压输注以及在维持麻醉的情况下从猪肠系膜上动脉(SMA)进行局部血管加压输注。实验 1 包括全强度(40%)抽血和全身血管加压(去甲肾上腺素和肾上腺素)。实验 2 包括全强度(40%)抽血、全身去甲肾上腺素和向 SMA 输注局部血管抑制剂。实验 3 涉及中度(27%)抽血、全身去甲肾上腺素输注和局部肾上腺素输注。我们对血清乳酸水平、肠道血清膜颜色、计算机断层扫描(CT)血管造影和病理结果进行了评估:结果:诱导出血后,单独使用全身血管加压素或联合使用局部血管加压素或去甲肾上腺素输注均不会诱导肠道缺血性颜色变化。中度(27% 失血量)出血后联合使用全身去甲肾上腺素和局部肾上腺素(0.5 μg/kg/min)可引起肠道颜色改变、病理破坏和血清乳酸升高。CT血管造影证实了SMA的通畅:我们建立了一个猪 NOMI 模型,在中度失血性休克时使用全身去甲肾上腺素输注和局部肾上腺素。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


