Arianna Burton, Yong Chen, Priya Patel, Jose Alvir, Darren Kailung Jeng, Anna Stachel Kane, Jiayin Xue, Emily Cibelli, Patrick F. Fogarty
{"title":"Multiyear, real-world, retrospective cohort study using a patient-centric approach to evaluate the burden of haemophilia B in the United States","authors":"Arianna Burton, Yong Chen, Priya Patel, Jose Alvir, Darren Kailung Jeng, Anna Stachel Kane, Jiayin Xue, Emily Cibelli, Patrick F. Fogarty","doi":"10.1111/hae.15077","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Haemophilia is associated with a high burden of illness. As disease severity worsens, people with haemophilia B (PwHB) experience greater loss of productivity, higher costs,<span><sup>1</sup></span> and reduced quality of life.<span><sup>2</sup></span> The hallmark of severe haemophilia is spontaneous bleeding into joints and muscles that may lead to long-term joint damage and pain.<span><sup>3</sup></span> The current standard of care for severe haemophilia B is prophylaxis with intravenous factor replacement therapy.<span><sup>3</sup></span> However, the treatment armamentarium for PwHB is expanding with investigational non-factor replacement therapies (anti-tissue factor pathway inhibitor, serpins, and small interfering RNA therapy targeting antithrombin) and advances in gene therapies.<span><sup>3, 4</sup></span></p><p>Real-world data (RWD) can help elucidate the burden of illness among PwHB and inform care decisions.<span><sup>1</sup></span> However, sources such as insurance claims are confined to billing codes and often lack data on disease severity and/or bleeding events.<span><sup>1</sup></span> Electronic health records (EHRs) contain narrative text with outcomes and disease characterisation data,<span><sup>5</sup></span> but information captured may vary between organisations and records are not always accessible electronically.<span><sup>6</sup></span></p><p>PicnicHealth is a novel patient-centric RWD platform incorporating multiyear, cross-institutional patient medical records (electronic and non-electronic). The PicnicHealth platform retrieves medical records directly from providers regardless of provider system, digitises medical records and produces a real-world dataset of a patient's medical journey. Clinical information is gathered retrospectively from structured and narrative sections of the medical records, digital imaging and communications in medicine images, medical and pharmacy claims and patient-reported outcomes.<span><sup>7</sup></span> We describe the results of a retrospective cohort study using longitudinal medical record data from PicnicHealth to assess the real-world burden of illness among PwHB in the United States.</p><p>From June 2020, PwHB (or their caregivers) were identified through social media outreach, provider partnerships, and patient advocacy groups. The study population included male PwHB who had medical records available between 1 April 2015 and 30 September 2020 (index date was the first encounter date in the dataset defined by haemophilia B diagnosis or factor IX [FIX] treatment). Exclusion criteria included recipients of any bypassing agent, inhibitor diagnosis (historical or current) and clinical trial enrolment. Data production and analysis are described in the Supplementary Methods. Descriptive statistics were reported for PwHB with data on annualised bleeding rate (ABR) after the index date. The cohort was stratified by disease severity, age (< 12 or ≥ 12 years old on index date), treatment regimen (prophylaxis or on demand) and body mass index (BMI).</p><p>Of 93 male PwHB identified within the PicnicHealth dataset, 75 were without inhibitors, not enrolled in a clinical trial and had documented disease severity. Of these, 48 had ABR data. Median (range) age was 21 (0−64) years; most patients were White (65%) and aged ≥ 12 years (73%) (Table 1). Haemophilia B was mild/moderate in 42% (<i>n </i>= 20/48) and severe in 58% (<i>n </i>= 28/48) of patients. Overall, 67% (<i>n </i>= 32/48) were receiving prophylaxis (75% [<i>n </i>= 24/32] of those had severe disease), 25% (<i>n </i>= 12/48) received on-demand treatment and 6% (<i>n </i>= 3/48) were not receiving a FIX replacement product. Treatment status was unknown for one patient. Prophylaxis use increased with disease severity; 40% (<i>n </i>= 8/20) of patients with mild/moderate disease used prophylaxis compared with 86% (<i>n </i>= 24/28) in those with severe disease.</p><p>The most frequent comorbid conditions were arthropathy (71%), synovitis (38%), mental and behavioural disorders (23%), diseases of the circulatory system (21%), and endocrine, nutritional, and metabolic diseases (23%). Comorbidities were reported in the same proportion (75%) of patients with mild/moderate and severe haemophilia B. Diseases of the musculoskeletal system (80% and 46%), arthropathy (80% and 46%) and synovitis (43% and 23%) were most frequently reported in patients aged ≥ 12 years and < 12 years, respectively. Pain medication was used by 88% of patients (93% with severe disease, 80% with mild/moderate disease), most commonly acetaminophen (83%) and celecoxib (25%).</p><p>Overall, 18/20 (90%) patients with mild/moderate disease and 27/28 (96%) with severe disease reported ≥1 bleeding event. ABR corresponded to disease severity; mean (median; interquartile range) ABR was 2.5 (1.3; 0−4.3) in patients with mild/moderate haemophilia B and 4.5 (1.5; 0−5.4) in those with severe disease (Figure 1A). These patterns were observed regardless of age group (< 12 years, Figure 1B; ≥ 12 years, Figure 1C). For those on prophylaxis, mean ABR was similar and median ABR was higher in patients with mild/moderate than severe disease (Figure 1D). ABR was generally higher in those with BMI outside the normal weight range, with a mean ABR of 2.4, 1.8, 4.5 and 6.8 in PwHB who were underweight (BMI <18.5 kg/m<sup>2</sup>; <i>n </i>= 9), normal weight (18.5−24.9 kg/m<sup>2</sup>; <i>n</i> = 17), overweight (25.0−29.9 kg/m<sup>2</sup>; <i>n </i>= 11) and obese (≥30 kg/m<sup>2</sup>; <i>n </i>= 11), respectively.</p><p>In this real-world cohort of PwHB, most patients (94%) reported ≥ 1 bleeding event. Disease burden was characterised by an increasing ABR associated with disease severity, numerous comorbid conditions and substantial use of pain medication. The Hemophilia Utilization Group Studies from 10 US-based haemophilia treatment centres (<i>n </i>= 112) also reported increases in ABR with disease severity: mean ABR was 3.5 (SD 5.1) and 7.1 (SD 7.7) for mild/moderate and severe disease, respectively.<span><sup>1</sup></span> In the ‘Cost of Haemophilia in Europe: a Socioeconomic Survey’ data set (CHESS II) from six European countries (<i>N </i>= 707), disease severity was associated with bleeding outcomes and was a significant predictor of increasing humanistic and economic burden.<span><sup>2</sup></span> In our study, prophylaxis use increased with disease severity. This is consistent with findings of a large study of prophylaxis in haemophilia B patients from the Centers for Disease Control and Prevention's Universal Data Collection project in the United States, where severity was strongly associated with prophylaxis use.<span><sup>8</sup></span></p><p>More severe diseases and age ≥ 12 years were associated with an increased rate of comorbid conditions, most notably arthropathy and synovitis. More than 80% of PwHB aged ≥ 12 years with severe disease experienced arthropathy. World Federation of Hemophilia guidance recognises that even with prophylaxis, clinical and subclinical bleeds cause progressive joint damage.<span><sup>3</sup></span> Mental and behavioural disorders occurred in 29% of PwHB with severe disease who were ≥ 12 years of age. Observations from the CHESS II dataset support these findings, with greater health-related quality of life impairments with increasing disease severity<span><sup>2</sup></span> and more annual bleeds.<span><sup>9</sup></span></p><p>The highest average ABR occurred in PwHB classified as obese or overweight; those classified as normal weight had the lowest ABR. Higher bleeding rates in those with obesity could be related to lower prophylaxis use,<span><sup>8</sup></span> as well as difficulties with venous access and ability to self-infuse.<span><sup>10</sup></span> However, there is some inconsistency between studies exploring bleeding and obesity, as other reports suggest patients with overweight/obesity have lower bleeding rates possibly due to reduction in physical activity.<span><sup>3</sup></span> Potential variability in levels of physical activity, intrinsic bleeding tendency and treatment characteristics limit the interpretability of these findings.</p><p>Pain medication was used frequently, with acetaminophen being the most common, particularly in patients < 12 years of age. Increased use of pain medication was observed with worsening disease severity, with celecoxib and acetaminophen more commonly used in patients with severe disease. In a subgroup analysis of adults with haemophilia A in CHESS II, pain and burden of disease increased with the number of bleeds.<span><sup>9</sup></span> This highlights the need for appropriate and timely treatment to avoid long-term joint damage and pain.<span><sup>3</sup></span></p><p>These findings need to be considered in the context of the study limitations, including relatively small sample sizes (especially for those < 12 years of age). Results may not be representative of those with milder disease severities given the high proportion of patients with severe disease included. Psychological diagnoses may be under-recorded, as providers may not release sensitive psychological diagnoses, especially in the paediatric population. Pain medication could be used for conditions other than haemophilia B or its complications. Patients self-select into the PicnicHealth platform, which could bias the study. Medical records may be irretrievable, lost or uninterpretable, causing gaps in longitudinal data. Bleeds that are minor or resolved quickly may be underreported in medical records. Clinical information on diagnoses and symptoms was gathered retrospectively and therefore relied upon accurate reporting, but there is potential for similar presentations such as synovitis and acute bleeds to be miscoded. Patients may not report all their providers, making data retrieval incomplete; however, PicnicHealth uses other information sources, such as claims linkage, to search for providers that are potentially missing. Finally, adult patient records do not always contain a date of diagnosis because severe haemophilia is usually diagnosed during infancy and most US states only guarantee healthcare data retention for up to 7 years, so some instances of burden faced during the period immediately following diagnosis (e.g., ABR, the effectiveness of treatment regimen, treatment switches) may not be captured.</p><p>Notably, 90% of patients with mild/moderate haemophilia B and 96% of those with severe disease reported ≥1 bleeding event. Pain medication was used in 88% of patients overall and 80% of those with mild/moderate disease. Overall, only 67% were receiving prophylaxis. These RWD demonstrate an ongoing burden from bleeding episodes, associated comorbidities, and pain medication use in a cohort of paediatric and adult PwHB, even among those using prophylaxis. These observations demonstrate current shortcomings in prevention of joint disease and underscore the need for enhanced use of prophylaxis and continued treatment advancements in haemophilia B.</p><p>Arianna Burton, Yong Chen, Priya Patel, and Patrick F. Fogarty conceptualized and designed the study, and analysed and interpreted the data. Yong Chen, Jose Alvir, Darren Kailung Jeng, Anna Stachel Kane, Jiayin Xue, and Emily Cibelli acquired, analysed, and interpreted the data. All authors participated in the critical review and final approval of the version to be submitted.</p><p>A.B., Y.C., P.P., and A.S.K. are employees of and own stocks and/or options in Pfizer. D.K.J. is an employee of Pfizer. J.A. and P.F.F. were employees of Pfizer at the time of this work and own stocks in Pfizer. J.X. was an employee of PicnicHealth at the time of this work. E.C. is an employee of PicnicHealth and owns stock options in PicnicHealth.</p><p>This study was sponsored by Pfizer.</p><p>Each PwHB (or their caregiver) signed a Health Insurance Portability and Accountability Act authorisation for PicnicHealth to contact their healthcare providers, retrieve their medical records and share their de-identified data for research. Records were collected from any US provider, at any healthcare facility caring for the patient. The study protocol and consent forms received institutional research board approval.</p>","PeriodicalId":12819,"journal":{"name":"Haemophilia","volume":"30 5","pages":"1234-1237"},"PeriodicalIF":3.0000,"publicationDate":"2024-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.15077","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Haemophilia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hae.15077","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Dear Editor,
Haemophilia is associated with a high burden of illness. As disease severity worsens, people with haemophilia B (PwHB) experience greater loss of productivity, higher costs,1 and reduced quality of life.2 The hallmark of severe haemophilia is spontaneous bleeding into joints and muscles that may lead to long-term joint damage and pain.3 The current standard of care for severe haemophilia B is prophylaxis with intravenous factor replacement therapy.3 However, the treatment armamentarium for PwHB is expanding with investigational non-factor replacement therapies (anti-tissue factor pathway inhibitor, serpins, and small interfering RNA therapy targeting antithrombin) and advances in gene therapies.3, 4
Real-world data (RWD) can help elucidate the burden of illness among PwHB and inform care decisions.1 However, sources such as insurance claims are confined to billing codes and often lack data on disease severity and/or bleeding events.1 Electronic health records (EHRs) contain narrative text with outcomes and disease characterisation data,5 but information captured may vary between organisations and records are not always accessible electronically.6
PicnicHealth is a novel patient-centric RWD platform incorporating multiyear, cross-institutional patient medical records (electronic and non-electronic). The PicnicHealth platform retrieves medical records directly from providers regardless of provider system, digitises medical records and produces a real-world dataset of a patient's medical journey. Clinical information is gathered retrospectively from structured and narrative sections of the medical records, digital imaging and communications in medicine images, medical and pharmacy claims and patient-reported outcomes.7 We describe the results of a retrospective cohort study using longitudinal medical record data from PicnicHealth to assess the real-world burden of illness among PwHB in the United States.
From June 2020, PwHB (or their caregivers) were identified through social media outreach, provider partnerships, and patient advocacy groups. The study population included male PwHB who had medical records available between 1 April 2015 and 30 September 2020 (index date was the first encounter date in the dataset defined by haemophilia B diagnosis or factor IX [FIX] treatment). Exclusion criteria included recipients of any bypassing agent, inhibitor diagnosis (historical or current) and clinical trial enrolment. Data production and analysis are described in the Supplementary Methods. Descriptive statistics were reported for PwHB with data on annualised bleeding rate (ABR) after the index date. The cohort was stratified by disease severity, age (< 12 or ≥ 12 years old on index date), treatment regimen (prophylaxis or on demand) and body mass index (BMI).
Of 93 male PwHB identified within the PicnicHealth dataset, 75 were without inhibitors, not enrolled in a clinical trial and had documented disease severity. Of these, 48 had ABR data. Median (range) age was 21 (0−64) years; most patients were White (65%) and aged ≥ 12 years (73%) (Table 1). Haemophilia B was mild/moderate in 42% (n = 20/48) and severe in 58% (n = 28/48) of patients. Overall, 67% (n = 32/48) were receiving prophylaxis (75% [n = 24/32] of those had severe disease), 25% (n = 12/48) received on-demand treatment and 6% (n = 3/48) were not receiving a FIX replacement product. Treatment status was unknown for one patient. Prophylaxis use increased with disease severity; 40% (n = 8/20) of patients with mild/moderate disease used prophylaxis compared with 86% (n = 24/28) in those with severe disease.
The most frequent comorbid conditions were arthropathy (71%), synovitis (38%), mental and behavioural disorders (23%), diseases of the circulatory system (21%), and endocrine, nutritional, and metabolic diseases (23%). Comorbidities were reported in the same proportion (75%) of patients with mild/moderate and severe haemophilia B. Diseases of the musculoskeletal system (80% and 46%), arthropathy (80% and 46%) and synovitis (43% and 23%) were most frequently reported in patients aged ≥ 12 years and < 12 years, respectively. Pain medication was used by 88% of patients (93% with severe disease, 80% with mild/moderate disease), most commonly acetaminophen (83%) and celecoxib (25%).
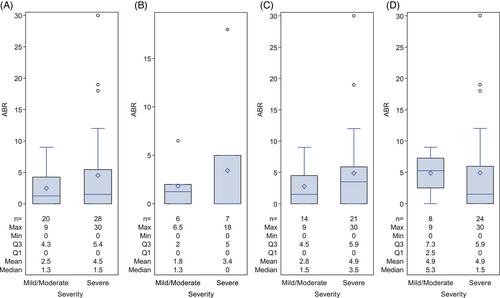
Overall, 18/20 (90%) patients with mild/moderate disease and 27/28 (96%) with severe disease reported ≥1 bleeding event. ABR corresponded to disease severity; mean (median; interquartile range) ABR was 2.5 (1.3; 0−4.3) in patients with mild/moderate haemophilia B and 4.5 (1.5; 0−5.4) in those with severe disease (Figure 1A). These patterns were observed regardless of age group (< 12 years, Figure 1B; ≥ 12 years, Figure 1C). For those on prophylaxis, mean ABR was similar and median ABR was higher in patients with mild/moderate than severe disease (Figure 1D). ABR was generally higher in those with BMI outside the normal weight range, with a mean ABR of 2.4, 1.8, 4.5 and 6.8 in PwHB who were underweight (BMI <18.5 kg/m2; n = 9), normal weight (18.5−24.9 kg/m2; n = 17), overweight (25.0−29.9 kg/m2; n = 11) and obese (≥30 kg/m2; n = 11), respectively.
In this real-world cohort of PwHB, most patients (94%) reported ≥ 1 bleeding event. Disease burden was characterised by an increasing ABR associated with disease severity, numerous comorbid conditions and substantial use of pain medication. The Hemophilia Utilization Group Studies from 10 US-based haemophilia treatment centres (n = 112) also reported increases in ABR with disease severity: mean ABR was 3.5 (SD 5.1) and 7.1 (SD 7.7) for mild/moderate and severe disease, respectively.1 In the ‘Cost of Haemophilia in Europe: a Socioeconomic Survey’ data set (CHESS II) from six European countries (N = 707), disease severity was associated with bleeding outcomes and was a significant predictor of increasing humanistic and economic burden.2 In our study, prophylaxis use increased with disease severity. This is consistent with findings of a large study of prophylaxis in haemophilia B patients from the Centers for Disease Control and Prevention's Universal Data Collection project in the United States, where severity was strongly associated with prophylaxis use.8
More severe diseases and age ≥ 12 years were associated with an increased rate of comorbid conditions, most notably arthropathy and synovitis. More than 80% of PwHB aged ≥ 12 years with severe disease experienced arthropathy. World Federation of Hemophilia guidance recognises that even with prophylaxis, clinical and subclinical bleeds cause progressive joint damage.3 Mental and behavioural disorders occurred in 29% of PwHB with severe disease who were ≥ 12 years of age. Observations from the CHESS II dataset support these findings, with greater health-related quality of life impairments with increasing disease severity2 and more annual bleeds.9
The highest average ABR occurred in PwHB classified as obese or overweight; those classified as normal weight had the lowest ABR. Higher bleeding rates in those with obesity could be related to lower prophylaxis use,8 as well as difficulties with venous access and ability to self-infuse.10 However, there is some inconsistency between studies exploring bleeding and obesity, as other reports suggest patients with overweight/obesity have lower bleeding rates possibly due to reduction in physical activity.3 Potential variability in levels of physical activity, intrinsic bleeding tendency and treatment characteristics limit the interpretability of these findings.
Pain medication was used frequently, with acetaminophen being the most common, particularly in patients < 12 years of age. Increased use of pain medication was observed with worsening disease severity, with celecoxib and acetaminophen more commonly used in patients with severe disease. In a subgroup analysis of adults with haemophilia A in CHESS II, pain and burden of disease increased with the number of bleeds.9 This highlights the need for appropriate and timely treatment to avoid long-term joint damage and pain.3
These findings need to be considered in the context of the study limitations, including relatively small sample sizes (especially for those < 12 years of age). Results may not be representative of those with milder disease severities given the high proportion of patients with severe disease included. Psychological diagnoses may be under-recorded, as providers may not release sensitive psychological diagnoses, especially in the paediatric population. Pain medication could be used for conditions other than haemophilia B or its complications. Patients self-select into the PicnicHealth platform, which could bias the study. Medical records may be irretrievable, lost or uninterpretable, causing gaps in longitudinal data. Bleeds that are minor or resolved quickly may be underreported in medical records. Clinical information on diagnoses and symptoms was gathered retrospectively and therefore relied upon accurate reporting, but there is potential for similar presentations such as synovitis and acute bleeds to be miscoded. Patients may not report all their providers, making data retrieval incomplete; however, PicnicHealth uses other information sources, such as claims linkage, to search for providers that are potentially missing. Finally, adult patient records do not always contain a date of diagnosis because severe haemophilia is usually diagnosed during infancy and most US states only guarantee healthcare data retention for up to 7 years, so some instances of burden faced during the period immediately following diagnosis (e.g., ABR, the effectiveness of treatment regimen, treatment switches) may not be captured.
Notably, 90% of patients with mild/moderate haemophilia B and 96% of those with severe disease reported ≥1 bleeding event. Pain medication was used in 88% of patients overall and 80% of those with mild/moderate disease. Overall, only 67% were receiving prophylaxis. These RWD demonstrate an ongoing burden from bleeding episodes, associated comorbidities, and pain medication use in a cohort of paediatric and adult PwHB, even among those using prophylaxis. These observations demonstrate current shortcomings in prevention of joint disease and underscore the need for enhanced use of prophylaxis and continued treatment advancements in haemophilia B.
Arianna Burton, Yong Chen, Priya Patel, and Patrick F. Fogarty conceptualized and designed the study, and analysed and interpreted the data. Yong Chen, Jose Alvir, Darren Kailung Jeng, Anna Stachel Kane, Jiayin Xue, and Emily Cibelli acquired, analysed, and interpreted the data. All authors participated in the critical review and final approval of the version to be submitted.
A.B., Y.C., P.P., and A.S.K. are employees of and own stocks and/or options in Pfizer. D.K.J. is an employee of Pfizer. J.A. and P.F.F. were employees of Pfizer at the time of this work and own stocks in Pfizer. J.X. was an employee of PicnicHealth at the time of this work. E.C. is an employee of PicnicHealth and owns stock options in PicnicHealth.
This study was sponsored by Pfizer.
Each PwHB (or their caregiver) signed a Health Insurance Portability and Accountability Act authorisation for PicnicHealth to contact their healthcare providers, retrieve their medical records and share their de-identified data for research. Records were collected from any US provider, at any healthcare facility caring for the patient. The study protocol and consent forms received institutional research board approval.
期刊介绍:
Haemophilia is an international journal dedicated to the exchange of information regarding the comprehensive care of haemophilia. The Journal contains review articles, original scientific papers and case reports related to haemophilia care, with frequent supplements. Subjects covered include:
clotting factor deficiencies, both inherited and acquired: haemophilia A, B, von Willebrand''s disease, deficiencies of factor V, VII, X and XI
replacement therapy for clotting factor deficiencies
component therapy in the developing world
transfusion transmitted disease
haemophilia care and paediatrics, orthopaedics, gynaecology and obstetrics
nursing
laboratory diagnosis
carrier detection
psycho-social concerns
economic issues
audit
inherited platelet disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


