A novel simplified sonographic approach with fluoroscopy-controlled L5 transforaminal epidural injections in patients with high iliac crest: a retrospective study.
{"title":"A novel simplified sonographic approach with fluoroscopy-controlled L5 transforaminal epidural injections in patients with high iliac crest: a retrospective study.","authors":"Haichang Yang, Hongyan Wang, Jie Lu, Ling Hu","doi":"10.1186/s40981-024-00725-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To explore a novel ultrasound (US) modality for lumbar transforaminal epidural injections (TFEIs) in patients with low back pain (LBP) and L5 radicular pain combined with high iliac crest (HIC).</p><p><strong>Methods: </strong>One-hundred and forty-one patients were retrospectively stratified into two groups based on the treatment they received: novel group, receiving US-guided and fluoroscopy (FL)-controlled TFEIs using a sagittal oblique approach between the superior articular process of L5 and S1, and control group, receiving US-guided TFEIs with conventional transverse approach combined with FL confirmation. Accuracy of contrast dispersing into lumbar epidural space was set as the primary endpoint. Radiation dosages, procedure time, numeric rating scale (NRS) scores, Modified Oswestry Disability Questionnaire (MODQ) scores, adverse events, and rescue analgesic requirement were also recorded. The generalized liner mixed model (GLMMs) was employed to compare the repeatedly measured variables between groups, taking individual confounding factors as covariance.</p><p><strong>Results: </strong>The accuracy of TFEIs was 92.8% and 65.2% in novel and control group, with a significant difference of 26.7% (95% CI: 15.4%, 39.8%) between two modalities (p < 0.001). Significant pain relief was observed in novel group as opposed to control group after one injection. Procedure time in novel group (8.4 ± 1.6 min) was shorter than control group (15.8 ± 3.5 min) (p < 0.001) with less radiation dosage (3047 ± 5670 vs. 8808 ± 1039 μGy/m<sup>2</sup>, p < 0.001). Significantly, lower incidence of L5 paresthesia occurred in novel group. Statistical differences of NRS scores between the novel and control group were reached at 1 week after procedure (1 (IQR: - 1-3) vs. 3 (IQR: - 1-7), p = 0.006), while not reached at both 1- (1 (IQR: 0-2) vs. 1 (IQR: - 1-3), p = 0.086) or 3-month follow-up (0 (IQR: - 1-1) vs. 1 (IQR: 0-2), p = 0.094). Both groups showed similar functional improvement (F = 0.103, p = 0.749) during follow-up.</p><p><strong>Conclusions: </strong>The novel sonographic technique provided superior accuracy needle placement and better pain-relieving effect through one injection as compared to the routine transverse approach. Consequently, in situations where the HIC imposed limitations for TFEIs performance on L5, the novel technique should be recommended to consider increasing accurate puncture, minimizing radiation exposure, consuming procedure time, and reducing the risk of neuraxial injury.</p>","PeriodicalId":14635,"journal":{"name":"JA Clinical Reports","volume":"10 1","pages":"43"},"PeriodicalIF":1.0000,"publicationDate":"2024-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11264496/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JA Clinical Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40981-024-00725-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To explore a novel ultrasound (US) modality for lumbar transforaminal epidural injections (TFEIs) in patients with low back pain (LBP) and L5 radicular pain combined with high iliac crest (HIC).
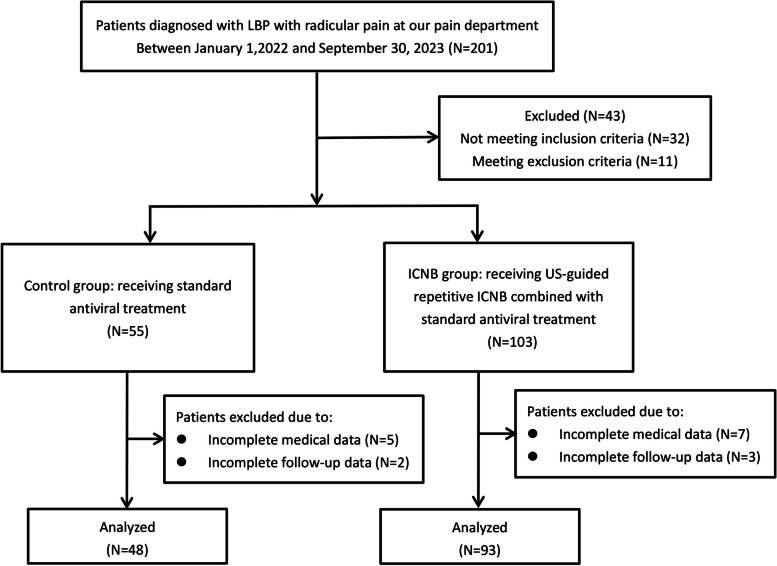
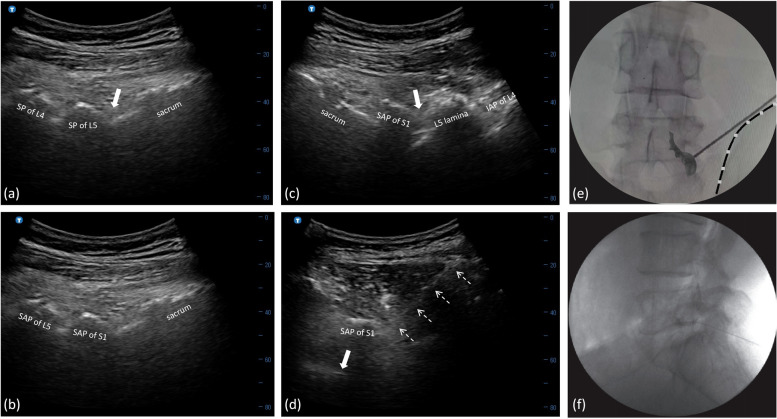
Methods: One-hundred and forty-one patients were retrospectively stratified into two groups based on the treatment they received: novel group, receiving US-guided and fluoroscopy (FL)-controlled TFEIs using a sagittal oblique approach between the superior articular process of L5 and S1, and control group, receiving US-guided TFEIs with conventional transverse approach combined with FL confirmation. Accuracy of contrast dispersing into lumbar epidural space was set as the primary endpoint. Radiation dosages, procedure time, numeric rating scale (NRS) scores, Modified Oswestry Disability Questionnaire (MODQ) scores, adverse events, and rescue analgesic requirement were also recorded. The generalized liner mixed model (GLMMs) was employed to compare the repeatedly measured variables between groups, taking individual confounding factors as covariance.
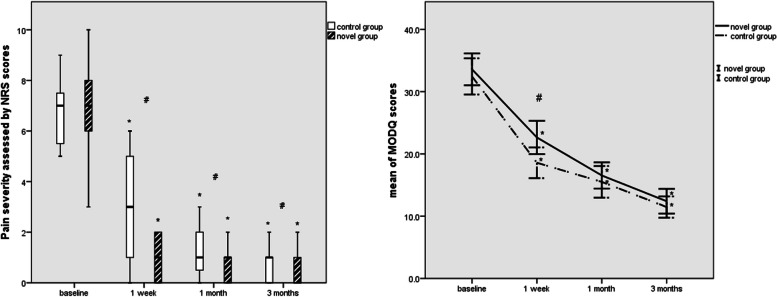
Results: The accuracy of TFEIs was 92.8% and 65.2% in novel and control group, with a significant difference of 26.7% (95% CI: 15.4%, 39.8%) between two modalities (p < 0.001). Significant pain relief was observed in novel group as opposed to control group after one injection. Procedure time in novel group (8.4 ± 1.6 min) was shorter than control group (15.8 ± 3.5 min) (p < 0.001) with less radiation dosage (3047 ± 5670 vs. 8808 ± 1039 μGy/m2, p < 0.001). Significantly, lower incidence of L5 paresthesia occurred in novel group. Statistical differences of NRS scores between the novel and control group were reached at 1 week after procedure (1 (IQR: - 1-3) vs. 3 (IQR: - 1-7), p = 0.006), while not reached at both 1- (1 (IQR: 0-2) vs. 1 (IQR: - 1-3), p = 0.086) or 3-month follow-up (0 (IQR: - 1-1) vs. 1 (IQR: 0-2), p = 0.094). Both groups showed similar functional improvement (F = 0.103, p = 0.749) during follow-up.
Conclusions: The novel sonographic technique provided superior accuracy needle placement and better pain-relieving effect through one injection as compared to the routine transverse approach. Consequently, in situations where the HIC imposed limitations for TFEIs performance on L5, the novel technique should be recommended to consider increasing accurate puncture, minimizing radiation exposure, consuming procedure time, and reducing the risk of neuraxial injury.
期刊介绍:
JA Clinical Reports is a companion journal to the Journal of Anesthesia (JA), the official journal of the Japanese Society of Anesthesiologists (JSA). This journal is an open access, peer-reviewed, online journal related to clinical anesthesia practices such as anesthesia management, pain management and intensive care. Case reports are very important articles from the viewpoint of education and the cultivation of scientific thinking in the field of anesthesia. However, submissions of anesthesia research and clinical reports from Japan are notably decreasing in major anesthesia journals. Therefore, the JSA has decided to launch a new journal, JA Clinical Reports, to encourage JSA members, particularly junior Japanese anesthesiologists, to publish papers in English language.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


