Kyung Hye Park, Jannet J Lee-Jayaram, Melissa K Kahili-Heede, Benjamin W Berg
{"title":"Simulation intervention related to family presence during resuscitation for physicians and medical students: a scoping review.","authors":"Kyung Hye Park, Jannet J Lee-Jayaram, Melissa K Kahili-Heede, Benjamin W Berg","doi":"10.15441/ceem.24.224","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Family presence during resuscitation (FPDR) is an established part of family-centered care. However, how physicians are educated about FPDR is relatively unclear. We aim to review the current status of FPDR simulation for physicians and medical students.</p><p><strong>Methods: </strong>A scoping review of literature published from 1999 to May 5, 2023, and written in English was undertaken. Articles were searched for using combinations of various family-, resuscitation-, and simulation-related words as keywords, respectively.</p><p><strong>Results: </strong>Eight articles were included in the final review. This review of FPDR simulation for physicians and medical students revealed findings in three categories: measuring cardiopulmonary resuscitation quality, investigating participant responses after FPDR simulation, and extracting exemplar good-communication elements. First, in four studies measuring resuscitation quality, physicians participated in adult resuscitation, and resuscitation quality was reduced with a family witness showing an overt reaction. Second, in three studies investigating the response to simulation training, interprofessional teams participating in pediatric resuscitation had negative responses to FPDR simulation. Third, in one study, good-communication elements during FPDR were observed during infant simulation, in which interprofessional teams participated. To the best of our knowledge, FPDR simulation training for medical students has not been reported.</p><p><strong>Conclusion: </strong>Our literature review highlights a gap in FPDR simulation involving physicians and/ or medical students. Physicians were more concerned with resuscitation quality than supporting families during resuscitation simulations. Medical students should be considered as participants for FPDR simulation. More high-evidence studies with interprofessional teams that include physicians and/or medical students are needed to evaluate curriculum design and participant-response changes following FPDR simulation.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"16-25"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010797/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.24.224","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Family presence during resuscitation (FPDR) is an established part of family-centered care. However, how physicians are educated about FPDR is relatively unclear. We aim to review the current status of FPDR simulation for physicians and medical students.
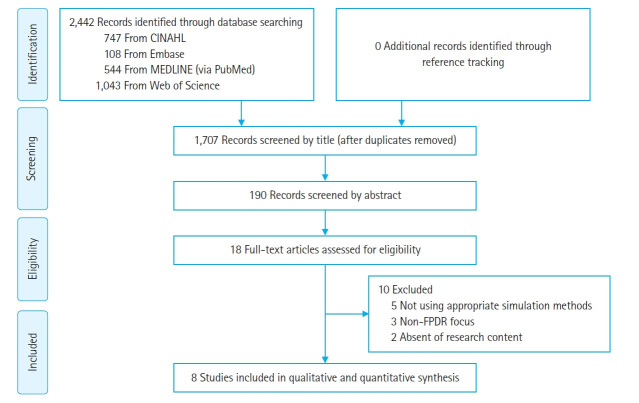
Methods: A scoping review of literature published from 1999 to May 5, 2023, and written in English was undertaken. Articles were searched for using combinations of various family-, resuscitation-, and simulation-related words as keywords, respectively.
Results: Eight articles were included in the final review. This review of FPDR simulation for physicians and medical students revealed findings in three categories: measuring cardiopulmonary resuscitation quality, investigating participant responses after FPDR simulation, and extracting exemplar good-communication elements. First, in four studies measuring resuscitation quality, physicians participated in adult resuscitation, and resuscitation quality was reduced with a family witness showing an overt reaction. Second, in three studies investigating the response to simulation training, interprofessional teams participating in pediatric resuscitation had negative responses to FPDR simulation. Third, in one study, good-communication elements during FPDR were observed during infant simulation, in which interprofessional teams participated. To the best of our knowledge, FPDR simulation training for medical students has not been reported.
Conclusion: Our literature review highlights a gap in FPDR simulation involving physicians and/ or medical students. Physicians were more concerned with resuscitation quality than supporting families during resuscitation simulations. Medical students should be considered as participants for FPDR simulation. More high-evidence studies with interprofessional teams that include physicians and/or medical students are needed to evaluate curriculum design and participant-response changes following FPDR simulation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


