Molecular relapse after first-line intensive therapy in patients with CBF or NPM1-mutated acute myeloid leukemia – a FILO study
IF 12.8
1区 医学
Q1 HEMATOLOGY
引用次数: 0
Abstract
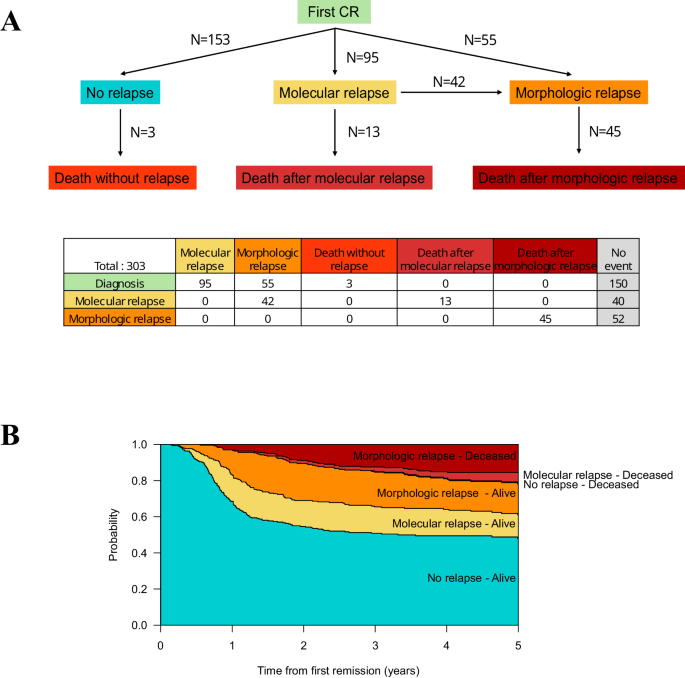
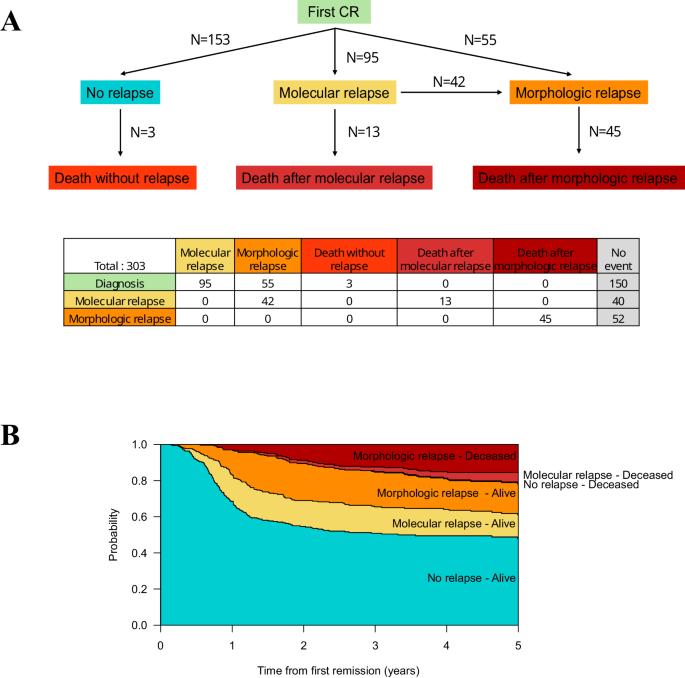
Patients with Core-Binding Factor (CBF) and NPM1-mutated acute myeloid leukemia (AML) can be monitored by quantitative PCR after having achieved first complete remission (CR) to detect morphologic relapse and drive preemptive therapy. How to best manage these patients is unknown. We retrospectively analyzed 303 patients with CBF and NPM1-mutated AML, aged 18–60 years, without allogeneic hematopoietic cell transplantation (HCT) in first CR, with molecular monitoring after first-line intensive therapy. Among these patients, 153 (51%) never relapsed, 95 (31%) had molecular relapse (53 received preemptive therapy and 42 progressed to morphologic relapse at salvage therapy), and 55 (18%) had upfront morphologic relapse. Patients who received preemptive therapy had higher OS than those who received salvage therapy after having progressed from molecular to morphologic relapse and those with upfront morphologic relapse (three-year OS: 78% vs. 51% vs. 51%, respectively, P = 0.01). Preemptive therapy included upfront allogeneic HCT (n = 19), intensive chemotherapy (n = 21), and non-intensive therapy (n = 13; three-year OS: 92% vs. 79% vs. 58%, respectively, P = 0.09). Although not definitive due to the non-randomized allocation of patients to different treatment strategies at relapse, our study suggests that molecular monitoring should be considered during follow-up to start preemptive therapy before overt morphologic relapse.
CBF或NPM1突变急性髓性白血病患者一线强化治疗后的分子复发--一项FILO研究
核心结合因子(CBF)和 NPM1 基因突变的急性髓性白血病(AML)患者在获得首次完全缓解(CR)后可通过定量 PCR 进行监测,以检测形态学复发并推动先期治疗。如何对这些患者进行最佳治疗尚不清楚。我们回顾性分析了 303 例 CBF 和 NPM1 基因突变的急性髓细胞性白血病患者,这些患者年龄在 18-60 岁之间,在首次 CR 时未接受异基因造血细胞移植 (HCT),并在一线强化治疗后接受了分子监测。在这些患者中,153人(51%)从未复发,95人(31%)出现分子复发(53人接受了先期治疗,42人在挽救治疗中进展为形态学复发),55人(18%)出现前期形态学复发。与分子复发进展到形态复发后接受挽救治疗的患者和前期形态复发的患者相比,接受先期治疗的患者的OS更高(三年OS:分别为78% vs. 51% vs. 51%,P = 0.01)。先期治疗包括前期异基因造血干细胞移植(19 例)、强化化疗(21 例)和非强化治疗(13 例;三年生存率分别为 92% vs. 79% vs. 58%,P = 0.09)。尽管由于在复发时将患者分配到不同治疗策略的非随机研究并不具有确定性,但我们的研究表明,在随访期间应考虑进行分子监测,以便在明显的形态学复发前开始先发制人的治疗。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Leukemia
医学-血液学
CiteScore
18.10
自引率
3.50%
发文量
270
审稿时长
3-6 weeks
期刊介绍:
Title: Leukemia
Journal Overview:
Publishes high-quality, peer-reviewed research
Covers all aspects of research and treatment of leukemia and allied diseases
Includes studies of normal hemopoiesis due to comparative relevance
Topics of Interest:
Oncogenes
Growth factors
Stem cells
Leukemia genomics
Cell cycle
Signal transduction
Molecular targets for therapy
And more
Content Types:
Original research articles
Reviews
Letters
Correspondence
Comments elaborating on significant advances and covering topical issues
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


