{"title":"To Evaluate Efficiency of Various Coronary Artery Disease Risk Scores With Traditional Risk Factors in Patients Undergoing Coronary Angiography.","authors":"Sharma Kamal, Panwar Jasraj, Patel Krutika, Parmar Devratsinh, Kalyani Maulik, Dhorajiya Dixit","doi":"10.37616/2212-5043.1386","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyze and compare various cardiovascular disease risk scores in Western Indian patients undergoing Coronary angiogram (CAG).</p><p><strong>Methods: </strong>In this prospective cross-sectional study, 1213 patients who underwent conventional coronary angiography; clinical risk profile and biochemical investigations were evaluated prior to undergoing CAG. Apart from the demographic information, 10-year absolute risk of having a major cardiovascular event (cardiovascular death, myocardial infarction or stroke) was calculated for each patient using various available Traditional Risk Scores (TRS). The population was divided in low, intermediate and high-risk categories for each of these scores.</p><p><strong>Results: </strong>Traditional cardiovascular risk factors like hypertension (41.8%) and diabetes mellitus-II (26.9%) were the two most prevalent risk factors in our study population. A higher risk value for all these TRS was more likely to be associated with obstructive coronary artery disease (OCAD) on CAG. Patients with high risk (≥20% for 10-year) QRESEARCH (QRISK3) score category had higher number of patients with obstructive CAD (49.6%) as compared to high risk category of risk score for those with high Global Registry of Acute Coronary Events (GRACE) score (46.6%) or risk Framingham (FRS CHD) score (29.2%) and risk atherosclerotic cardiovascular disease (ASCVD) score (30.1%) (P < 0.0001). A higher TRS was more likely to be associated with obstructive CAD, with the highest predictability being with QRISK3 (QRISK3 score 60.9%, GRACE score 54.9%, FRS-CHD score 34% and ASCVD score 42.1% respectively; P < 0.0001). A substantial study population (27.4%) cannot be identified using any of these TRS and hence a need of indigenous or modified risk scores is proposed.</p><p><strong>Conclusion: </strong>QRISK3 score was most efficacious for predicting obstructive CAD in our Indian study population on CAG. A higher risk score also correlated with the number of vessels involved on coronary angiogram. A substantial obstructive CAD patient could not be identified using traditional risk scores hence need for an indigenous or modified score.</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"36 2","pages":"128-136"},"PeriodicalIF":1.3000,"publicationDate":"2024-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11249062/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1386","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To analyze and compare various cardiovascular disease risk scores in Western Indian patients undergoing Coronary angiogram (CAG).
Methods: In this prospective cross-sectional study, 1213 patients who underwent conventional coronary angiography; clinical risk profile and biochemical investigations were evaluated prior to undergoing CAG. Apart from the demographic information, 10-year absolute risk of having a major cardiovascular event (cardiovascular death, myocardial infarction or stroke) was calculated for each patient using various available Traditional Risk Scores (TRS). The population was divided in low, intermediate and high-risk categories for each of these scores.
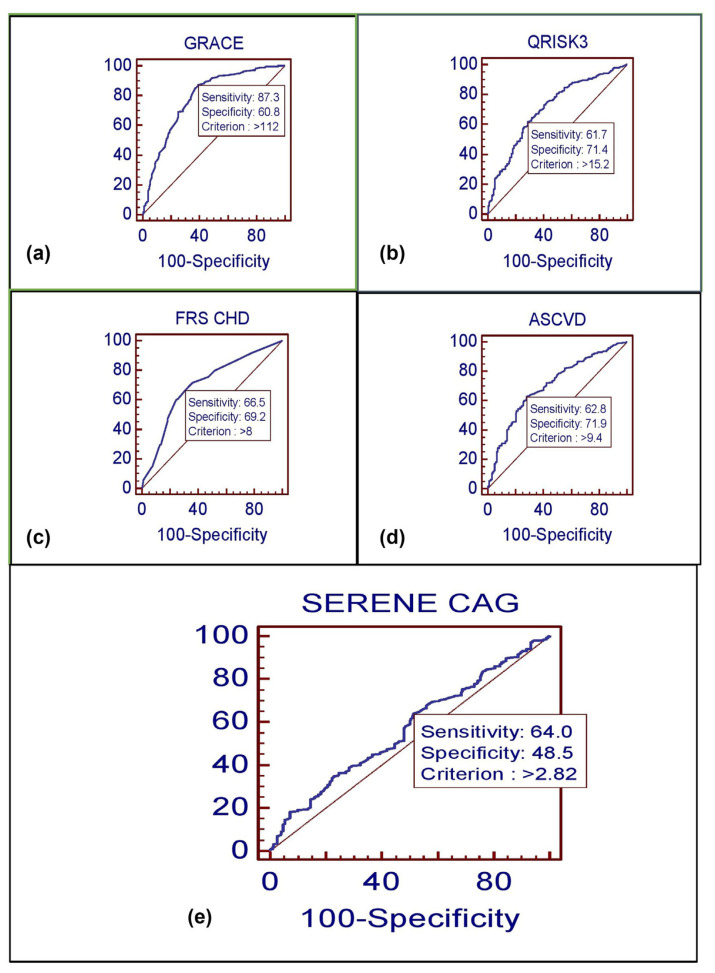
Results: Traditional cardiovascular risk factors like hypertension (41.8%) and diabetes mellitus-II (26.9%) were the two most prevalent risk factors in our study population. A higher risk value for all these TRS was more likely to be associated with obstructive coronary artery disease (OCAD) on CAG. Patients with high risk (≥20% for 10-year) QRESEARCH (QRISK3) score category had higher number of patients with obstructive CAD (49.6%) as compared to high risk category of risk score for those with high Global Registry of Acute Coronary Events (GRACE) score (46.6%) or risk Framingham (FRS CHD) score (29.2%) and risk atherosclerotic cardiovascular disease (ASCVD) score (30.1%) (P < 0.0001). A higher TRS was more likely to be associated with obstructive CAD, with the highest predictability being with QRISK3 (QRISK3 score 60.9%, GRACE score 54.9%, FRS-CHD score 34% and ASCVD score 42.1% respectively; P < 0.0001). A substantial study population (27.4%) cannot be identified using any of these TRS and hence a need of indigenous or modified risk scores is proposed.
Conclusion: QRISK3 score was most efficacious for predicting obstructive CAD in our Indian study population on CAG. A higher risk score also correlated with the number of vessels involved on coronary angiogram. A substantial obstructive CAD patient could not be identified using traditional risk scores hence need for an indigenous or modified score.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


