Frank G. Rücker, Andrea Corbacioglu, Julia Krzykalla, Sibylle Cocciardi, Claudia Lengerke, Ulrich Germing, Gerald Wulf, Maisun A. Samra, Lino L. Teichmann, Michael Lübbert, Michael W. M. Kühn, Martin Bentz, Jörg Westermann, Lars Bullinger, Verena I. Gaidzik, Annika Meid, Sophia Aicher, Frank Stegelmann, Daniela Weber, Anika Schrade, Felicitas Thol, Michael Heuser, Arnold Ganser, Axel Benner, Hartmut Döhner, Konstanze Döhner, for the German-Austrian Acute Myeloid Leukemia Study Group (AMLSG)
{"title":"Refinement of the prognostic impact of somatic CEBPA bZIP domain mutations in acute myeloid leukemia: Results of the AML Study Group (AMLSG)","authors":"Frank G. Rücker, Andrea Corbacioglu, Julia Krzykalla, Sibylle Cocciardi, Claudia Lengerke, Ulrich Germing, Gerald Wulf, Maisun A. Samra, Lino L. Teichmann, Michael Lübbert, Michael W. M. Kühn, Martin Bentz, Jörg Westermann, Lars Bullinger, Verena I. Gaidzik, Annika Meid, Sophia Aicher, Frank Stegelmann, Daniela Weber, Anika Schrade, Felicitas Thol, Michael Heuser, Arnold Ganser, Axel Benner, Hartmut Döhner, Konstanze Döhner, for the German-Austrian Acute Myeloid Leukemia Study Group (AMLSG)","doi":"10.1002/hem3.123","DOIUrl":null,"url":null,"abstract":"<p>The transcription factor CCAAT/enhancer binding protein alpha (CEBPA) is a key regulator of myelopoiesis and granulocyte differentiation.<span><sup>1, 2</sup></span> The intronless <i>CEBPA</i> gene on chromosome 19q13.1 encodes two DNA-binding protein isoforms: a full-length 42-kDa protein (p42) and a shorter 30-kDa isoform (p30), initiated from two distinct start sites.<span><sup>2</sup></span> The p42 isoform contains two N-terminal transactivation domains (TAD1, TAD2), whereas the p30 isoform lacks TAD1. Both isoforms contain the highly conserved C-terminal basic DNA-binding domain and the leucine zipper (bZIP) involved in DNA binding and protein dimerization. In younger adult patients, mutations of <i>CEBPA</i> (<i>CEBPA</i><sup>mut</sup>) are present in 5%–10% of newly diagnosed acute myeloid leukemia (AML); the frequency in older patients is considerably lower.<span><sup>2-5</sup></span> There are two mutational patterns: the first one clusters at the N-terminus involving the two TADs, typically frame-shift mutations; the second one at the C-terminus affecting bZIP, typically in-frame mutations. Out-of-frame TAD mutations result in the truncated p30 isoform that has been shown to act as a dominant negative of the p42 isoform and to be associated with increased proliferation and minimal differentiation of myeloid progenitors.<span><sup>2, 6</sup></span> Depending on the position, in-frame bZIP mutations cause a p42 isoform defective either in DNA binding or homo- and heterodimerization.<span><sup>3, 7</sup></span></p><p>Approximately half of the <i>CEBPA</i><sup>mut</sup> AML exhibit biallelic mutations (<i>CEBPA</i><sup>bi</sup>), typically consisting of one TAD and one bZIP mutation on separate alleles.<span><sup>3, 4</sup></span> Based on specific genetic features and its prognostic impact, <i>CEBPA</i><sup>bi</sup> was defined as a distinct entity within the 2016 WHO classification and was categorized as favorable in the risk stratification of the 2017 European LeukemiaNet (ELN) recommendations. Recent studies in pediatric and adult AML have demonstrated <i>CEBPA</i><sup>bZIP</sup> mutations, and in particular, in-frame mutations (<i>CEBPA</i><sup>bZIP_inf</sup>), to be associated with a unique gene-expression profile and favorable outcome, regardless of the mono- or biallelic status.<span><sup>8-10</sup></span> Based on these data, the former entity of AML with <i>CEBPA</i><sup>bi</sup> was expanded by single mutations in bZIP (smbZIP-<i>CEBPA</i>) in the current 2022 WHO classification and replaced by AML with <i>CEBPA</i><sup>bZIP_inf</sup> (irrespective of the allelic status) within the 2022 International Consensus Classification (ICC) of myeloid neoplasm and acute leukemias.<span><sup>11, 12</sup></span> Furthermore, <i>CEBPA</i><sup>bZIP_inf</sup> (irrespective of the allelic status) is now categorized as favorable in the 2022 ELN risk stratification.<span><sup>13</sup></span></p><p>To evaluate the prognostic impact of <i>CEBPA</i><sup>bZIP</sup>, in particular to further characterize <i>CEBPA</i><sup>bZIP_inf</sup> mutations, we retrospectively analyzed 528 intensively treated adult <i>CEBPA</i><sup>mut</sup> AML patients (median age: 54 years, range: 18–82; ≤60 years: <i>n</i> = 340, >60 years: <i>n</i> = 188) enrolled in treatment trials of the German-Austrian AML Study Group (AMLSG) and/or entered into the AMLSG BiO Registry study (NCT01252485). <i>CEBPA</i> mutation status was evaluated centrally in two reference laboratories of the AMLSG; assays were harmonized and cross-validated between the two laboratories. Sequences were analyzed for type of <i>CEBPA</i> mutations (insertions/deletions either in-frame or frameshift, missense, and nonsense mutations), the precise localization of mutations (TAD1/2 and bZIP), and allelic status. Two hundred forty-three (46%) patients were enrolled in one of 12 AMLSG treatment trials (Supporting Information S1: Appendix) and 285 (54%) received intensive treatment according to the standard of care. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent for treatment and genetic testing was obtained from all patients.</p><p>Complete remission (CR), including CR with incomplete hematologic recovery during induction cycles 1 and 2, was achieved in 425/501 (85%) evaluable patients. Allogeneic hematopoietic-cell transplantation (HCT) in the first CR (CR1) was performed in 109 (21%) patients. The median follow-up time was 55.5 months (95% confidence interval [95% CI], 51.2–59.5). Median event-free survival (EFS) and median overall survival (OS) were 20.0 (95% CI: 14.4–30.6) and 172.4 months (95% CI: 72.5–NA), respectively. The 5-year EFS and OS rates were 42% and 55%, respectively. One hundred forty-one (26.7%) patients relapsed, and 195 (36.9%) died.</p><p>Of the 528 patients, 263 (49.8%) exhibited ≥2 <i>CEBPA</i> mutations (dm<i>CEBPA</i>), and 265 had monoallelic <i>CEBPA</i> mutations (sm<i>CEBPA</i>). To further refine <i>CEBPA</i> mutation types and to address their prognostic impact, patients were categorized into eight groups based on allelic status (dm<i>CEBPA</i> vs. sm<i>CEBPA</i>) and mutation type: (1) dm<i>CEBPA</i> with in-frame insertion/deletion in bZIP (dm<i>CEBPA</i><sup>bZIP_InDel_inf</sup>, <i>n</i> = 220), (2) frame-shift insertion/deletion or nonsense mutation in bZIP (dm<i>CEBPA</i><sup>bZIP_InDel_fs</sup>, <i>n</i> = 13), (3) missense mutation in bZIP (dm<i>CEBPA</i><sup>bZIP_ms</sup>, <i>n</i> = 22), (4) other (dm<i>CEBPA</i><sup>other</sup>, <i>n</i> = 8), (5) sm<i>CEBPA</i><sup>bZIP_InDel_inf</sup> (<i>n</i> = 46), (6) sm<i>CEBPA</i><sup>bZIP_InDel_fs</sup> (<i>n</i> = 32), (7) sm<i>CEBPA</i><sup>bZIP_ms</sup> (<i>n</i> = 11), or (8) sm<i>CEBPA</i><sup>other</sup> (<i>n</i> = 176). These eight groups differed significantly with regard to several clinical and concurrent genetic features as well as achievement of CR1 and outcome (Supporting Information S1: Table 1).</p><p>To evaluate the prognostic impact of the eight <i>CEBPA</i> mutation types, we performed conditional inference tree models for EFS and OS. Of the eight equally relevant groups, dm<i>CEBPA</i><sup>bZIP_InDel_inf</sup> and sm<i>CEBPA</i><sup>bZIP_InDel_inf</sup> patients separated from the other groups in the first tree based on significantly lower cumulative incidences of events (refractory disease, relapse, and/or death). No further partitioning was observed (Supporting Information S1: Figure 1). Assuming a prognostic impact primarily for mutation type rather than allelic status, subsequent conditional inference tree models were performed by splitting up <i>CEBPA</i> mutation types and allelic status for EFS and OS. In both the models, the <i>CEBPA</i><sup>bZIP_InDel_inf</sup> group again separated significantly from the other three groups in the first tree without further separation, confirming the significantly favorable prognosis, regardless of the allelic status (Figure 1A and Supporting Information S1: Figure 2).</p><p>Based on these findings, patients were subsequently categorized as <i>CEBPA</i><sup>bZIP_InDel_inf</sup> (<i>n</i> = 266), <i>CEBPA</i><sup>bZIP_InDel_fs</sup> (<i>n</i> = 45), <i>CEBPA</i><sup>bZIP_ms</sup> (<i>n</i> = 33), or <i>CEBPA</i><sup>other</sup> (<i>n</i> = 184), irrespective of the allelic status. These four groups differed significantly with regard to several clinical and concurrent genetic features as well as achievement of CR1. Most obviously, <i>CEBPA</i><sup>bZIP_InDel_inf</sup> patients were younger (median age in years: 49 vs. 66 vs. 60 vs 61; <i>p</i> < .001) and achieved a higher CR1 rate (91.4% vs. 81.8% vs. 83.3% vs. 76.2%; <i>p</i> < .001) (Supporting Information S1: Table 2). Irrespective of the allelic status, <i>CEBPA</i><sup>bZIP_InDel_inf</sup> patients had a significantly improved EFS (median [95% CI] 49.8 months [16.9–82.7] vs. 11.5 [8.3–14.6] for <i>CEBPA</i><sup>bZIP_InDel_fs</sup> vs. 12.6 [6.2–19.1] for <i>CEBPA</i><sup>bZIP_ms</sup> vs 14.6 [7.7–21.5] for <i>CEBPA</i><sup>other</sup>; <i>p</i> < .001) and OS (median [95% CI] NA for patients with <i>CEBPA</i><sup>bZIP_InDel_inf</sup> [NA–NA] vs. 25.7 months [10.2–41.3] for <i>CEBPA</i><sup>bZIP_InDel_fs</sup> vs. 54.3 [14.6–NA] for <i>CEBPA</i><sup>bZIP_ms</sup> vs. 45.5 [13.1–77.9] for <i>CEBPA</i><sup>other</sup>; <i>p</i> < .001) (Figure 1B,C). Of note, a sensitivity analysis in which survival times were censored at the date of HCT in CR1 revealed almost identical results (Supporting Information S1: Figure 3).</p><p>Multivariate Cox models for EFS and OS adjusted for sex, type of AML, <i>FLT3</i>-ITD, <i>NPM1</i> mutation status, white blood cell (WBC) count (log10 transformed), bone marrow blasts, and age including HCT in CR1 as a time-dependent variable (Supporting Information S1: Appendix) revealed increasing age and higher WBC as unfavorable factors, whereas <i>CEBPA</i><sup>bZIP_InDel_inf</sup>, <i>NPM1</i><sup>mut</sup>, and HCT in CR1 were favorable (Table 1).</p><p>A recent meta-analysis of 1010 adult <i>CEBPA</i><sup>mut</sup> AML from six different study groups characterized <i>CEBPA</i> mutational subgroups in more detail by evaluating their clinical and genetic features as well as their prognostic impact.<span><sup>14</sup></span> In line with our data, the authors showed that <i>CEBPA</i><sup>bZIP_InDel_inf</sup> mutations represent a subset of AML with distinct disease biology and clinical outcomes. Despite certain limitations, in particular, the retrospective nature spanning almost three decades with evolving different treatment approaches, both studies independently confirm the less favorable impact of in-frame bZIP missense mutations (currently subsumed in the category AML with <i>CEBPA</i><sup>bZIP_inf</sup> in the ICC and ELN risk classification). The less favorable impact of bZIP missense mutations might be explained by the finding that bZIP missense mutations localize differently and therefore have diverse functional consequences. <i>CEBPA</i><sup>bZIP_InDel_inf</sup> predominantly affects the fork region of bZIP, while <i>CEBPA</i><sup>bZIP_ms</sup> cluster in the basic region (Supporting Information S1: Figure 4). These different mutation patterns imply that <i>CEBPA</i><sup>bZIP_ms</sup> impair DNA binding, while <i>CEBPA</i><sup>bZIP_InDel_inf</sup> affects dimerization. Murine data have shown that missense mutations in the basic region of bZIP lead to a myeloproliferative disease transforming into overt AML,<span><sup>7</sup></span> while AML arises upon transplantation of transgenic cells carrying the most common in-frame insertion in bZIP (K313dup, K-allele) alone or in combination with an N-terminal mutation (L-allele), with the K/L combination driving the most aggressive AML.<span><sup>15</sup></span></p><p>In this retrospective, exploratory analysis of 528 adult patients with newly diagnosed intensively treated patients with <i>CEBPA</i><sup>mut</sup> AML, we further refined the prognostic impact of different <i>CEBPA</i> mutation types, in particular, <i>CEBPA</i> mutations that are located in the bZIP domain. Our study shows that the beneficial effect is restricted to <i>CEBPA</i> bZIP InDel in-frame mutations, irrespective of the allelic status, whereas <i>CEBPA</i> bZIP missense mutations are associated with inferior outcomes. Our data as well as the data from Georgi et al. provide novel and clinically relevant results contributing to a further refinement of <i>CEBPA</i><sup>mut</sup> AML in the current ICC and WHO classifications as well as for risk stratification as recommended by the ELN.</p><p>Frank G. Rücker, Andrea Corbacioglu, Hartmut Döhner, and Konstanze Döhner designed the study. Frank G. Rücker, Andrea Corbacioglu, Sibylle Cocciardi, Verena I. Gaidzik, Annika Meid, and Sophia Aicher performed experiments and validated data. Frank G. Rücker, Julia Krzykalla, Daniela Weber, and Axel Benner performed statistical analyses. Frank G. Rücker, Andrea Corbacioglu, Julia Krzykalla, Daniela Weber, Axel Benner, Hartmut Döhner, and Konstanze Döhner analyzed the results. Claudia Lengerke, Ulrich Germing, Gerald Wulf, Maisun A. Samra, Lino L. Teichmann, Michael Lübbert, Michael W. M. Kühn, Martin Bentz, Jörg Westermann, Lars Bullinger, Frank Stegelmann, Anika Schrade, Felicitas Thol, Michael Heuser, and Arnold Ganser collected and provided patient samples and clinical information. Frank G. Rücker, Andrea Corbacioglu, Hartmut Döhner, and Konstanze Döhner wrote the first draft of the manuscript; and all authors undertook manuscript writing, editing, and approval, revised the manuscript, and reviewed and approved the final version.</p><p>Frank G. Rücker reports honoraria from and consultancy for Jazz Pharmaceuticals, Novartis, and BMS/Celgene; travel support from Jazz Pharmaceuticals. Michael Lübbert reports an advisory role for Abbvie, Astex Pharmaceuticals, Imago BioSciences, Janssen, Otsuka, and Syros; research support from Janssen and Cheplapharm. Michael W. M. Kühn reports honoraria from and consultancy for Pfizer, Kura Oncology, Jazz Pharmaceuticals, BMS/Celgene, and Abbvie; speakers bureau of Gilead. Lars Bullinger reports honoraria from Abbvie, Amgen, Astellas, BMS/Celgene, Daiichi Sankyo, Gilead, Janssen, Jazz Pharmaceuticals, Menarini, Novartis, Pfizer, Roche, and Sanofi; research support from Bayer and Jazz Pharmaceuticals. Verena I. Gaidzik reports an advisory role for Jazz Pharmaceuticals, Abbvie, and Boehringer-Ingelheim; speakers bureau of Pfizer, Janssen, and Abbvie; and travel support from Abbvie. Frank Stegelmann reports honoraria from and consultancy for AOP Pharma, MorphoSys, BMS/Celgene, Incyte, Novartis, and Pfizer. Felicitas Thol reports an advisory role for Novartis, BMS, Abbvie, Menarini, and Rigel. Michael Heuser reports honoraria from Certara, Jazz Pharmaceuticals, Janssen, Novartis, and Sobi; paid consultancy for Abbvie, Amgen, BMS/Celgene, Glycostem, LabDelbert, Pfizer, PinotBio, and Servier; and research funding to his institution from Abbvie, Agios, Astellas, BMS/Celgene, Glycostem, Jazz Pharmaceuticals, Karyopharm, Loxo Oncology, and PinotBio. Hartmut Döhner declares being in an advisory role for Abbvie, Agios, Amgen, Astellas, AstraZeneca, Berlin Chemie, BMS/Celgene, Daiichi Sankyo, GEMoaB, Gilead, Janssen, Jazz Pharmaceuticals, Novartis, Servier, Stemline, and Syndax; research funding from Abbvie, Agios, Amgen, Astellas, BMS/Celgene, Jazz Pharmaceuticals, Kronos Bio, Novartis, and Pfizer. Konstanze Döhner reports an advisory role for Amgen, BMS/Celgene, Daiichi Sankyo, Janssen, Jazz Pharmaceuticals, Novartis, and Roche; research funding from Agios, Astex, Astellas, BMS/Celgene, and Novartis. All other authors declare no competing interest. The remaining authors declared no conflicts of interest.</p><p>This work was supported in part by Collaborative Research Center SFB 1074, projects B3 and B12 (K.D.) and project Z1 (H.D.).</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11247273/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.123","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
The transcription factor CCAAT/enhancer binding protein alpha (CEBPA) is a key regulator of myelopoiesis and granulocyte differentiation.1, 2 The intronless CEBPA gene on chromosome 19q13.1 encodes two DNA-binding protein isoforms: a full-length 42-kDa protein (p42) and a shorter 30-kDa isoform (p30), initiated from two distinct start sites.2 The p42 isoform contains two N-terminal transactivation domains (TAD1, TAD2), whereas the p30 isoform lacks TAD1. Both isoforms contain the highly conserved C-terminal basic DNA-binding domain and the leucine zipper (bZIP) involved in DNA binding and protein dimerization. In younger adult patients, mutations of CEBPA (CEBPAmut) are present in 5%–10% of newly diagnosed acute myeloid leukemia (AML); the frequency in older patients is considerably lower.2-5 There are two mutational patterns: the first one clusters at the N-terminus involving the two TADs, typically frame-shift mutations; the second one at the C-terminus affecting bZIP, typically in-frame mutations. Out-of-frame TAD mutations result in the truncated p30 isoform that has been shown to act as a dominant negative of the p42 isoform and to be associated with increased proliferation and minimal differentiation of myeloid progenitors.2, 6 Depending on the position, in-frame bZIP mutations cause a p42 isoform defective either in DNA binding or homo- and heterodimerization.3, 7
Approximately half of the CEBPAmut AML exhibit biallelic mutations (CEBPAbi), typically consisting of one TAD and one bZIP mutation on separate alleles.3, 4 Based on specific genetic features and its prognostic impact, CEBPAbi was defined as a distinct entity within the 2016 WHO classification and was categorized as favorable in the risk stratification of the 2017 European LeukemiaNet (ELN) recommendations. Recent studies in pediatric and adult AML have demonstrated CEBPAbZIP mutations, and in particular, in-frame mutations (CEBPAbZIP_inf), to be associated with a unique gene-expression profile and favorable outcome, regardless of the mono- or biallelic status.8-10 Based on these data, the former entity of AML with CEBPAbi was expanded by single mutations in bZIP (smbZIP-CEBPA) in the current 2022 WHO classification and replaced by AML with CEBPAbZIP_inf (irrespective of the allelic status) within the 2022 International Consensus Classification (ICC) of myeloid neoplasm and acute leukemias.11, 12 Furthermore, CEBPAbZIP_inf (irrespective of the allelic status) is now categorized as favorable in the 2022 ELN risk stratification.13
To evaluate the prognostic impact of CEBPAbZIP, in particular to further characterize CEBPAbZIP_inf mutations, we retrospectively analyzed 528 intensively treated adult CEBPAmut AML patients (median age: 54 years, range: 18–82; ≤60 years: n = 340, >60 years: n = 188) enrolled in treatment trials of the German-Austrian AML Study Group (AMLSG) and/or entered into the AMLSG BiO Registry study (NCT01252485). CEBPA mutation status was evaluated centrally in two reference laboratories of the AMLSG; assays were harmonized and cross-validated between the two laboratories. Sequences were analyzed for type of CEBPA mutations (insertions/deletions either in-frame or frameshift, missense, and nonsense mutations), the precise localization of mutations (TAD1/2 and bZIP), and allelic status. Two hundred forty-three (46%) patients were enrolled in one of 12 AMLSG treatment trials (Supporting Information S1: Appendix) and 285 (54%) received intensive treatment according to the standard of care. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent for treatment and genetic testing was obtained from all patients.
Complete remission (CR), including CR with incomplete hematologic recovery during induction cycles 1 and 2, was achieved in 425/501 (85%) evaluable patients. Allogeneic hematopoietic-cell transplantation (HCT) in the first CR (CR1) was performed in 109 (21%) patients. The median follow-up time was 55.5 months (95% confidence interval [95% CI], 51.2–59.5). Median event-free survival (EFS) and median overall survival (OS) were 20.0 (95% CI: 14.4–30.6) and 172.4 months (95% CI: 72.5–NA), respectively. The 5-year EFS and OS rates were 42% and 55%, respectively. One hundred forty-one (26.7%) patients relapsed, and 195 (36.9%) died.
Of the 528 patients, 263 (49.8%) exhibited ≥2 CEBPA mutations (dmCEBPA), and 265 had monoallelic CEBPA mutations (smCEBPA). To further refine CEBPA mutation types and to address their prognostic impact, patients were categorized into eight groups based on allelic status (dmCEBPA vs. smCEBPA) and mutation type: (1) dmCEBPA with in-frame insertion/deletion in bZIP (dmCEBPAbZIP_InDel_inf, n = 220), (2) frame-shift insertion/deletion or nonsense mutation in bZIP (dmCEBPAbZIP_InDel_fs, n = 13), (3) missense mutation in bZIP (dmCEBPAbZIP_ms, n = 22), (4) other (dmCEBPAother, n = 8), (5) smCEBPAbZIP_InDel_inf (n = 46), (6) smCEBPAbZIP_InDel_fs (n = 32), (7) smCEBPAbZIP_ms (n = 11), or (8) smCEBPAother (n = 176). These eight groups differed significantly with regard to several clinical and concurrent genetic features as well as achievement of CR1 and outcome (Supporting Information S1: Table 1).
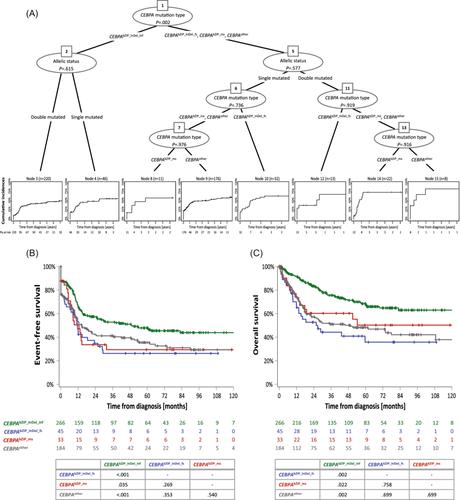
To evaluate the prognostic impact of the eight CEBPA mutation types, we performed conditional inference tree models for EFS and OS. Of the eight equally relevant groups, dmCEBPAbZIP_InDel_inf and smCEBPAbZIP_InDel_inf patients separated from the other groups in the first tree based on significantly lower cumulative incidences of events (refractory disease, relapse, and/or death). No further partitioning was observed (Supporting Information S1: Figure 1). Assuming a prognostic impact primarily for mutation type rather than allelic status, subsequent conditional inference tree models were performed by splitting up CEBPA mutation types and allelic status for EFS and OS. In both the models, the CEBPAbZIP_InDel_inf group again separated significantly from the other three groups in the first tree without further separation, confirming the significantly favorable prognosis, regardless of the allelic status (Figure 1A and Supporting Information S1: Figure 2).
Based on these findings, patients were subsequently categorized as CEBPAbZIP_InDel_inf (n = 266), CEBPAbZIP_InDel_fs (n = 45), CEBPAbZIP_ms (n = 33), or CEBPAother (n = 184), irrespective of the allelic status. These four groups differed significantly with regard to several clinical and concurrent genetic features as well as achievement of CR1. Most obviously, CEBPAbZIP_InDel_inf patients were younger (median age in years: 49 vs. 66 vs. 60 vs 61; p < .001) and achieved a higher CR1 rate (91.4% vs. 81.8% vs. 83.3% vs. 76.2%; p < .001) (Supporting Information S1: Table 2). Irrespective of the allelic status, CEBPAbZIP_InDel_inf patients had a significantly improved EFS (median [95% CI] 49.8 months [16.9–82.7] vs. 11.5 [8.3–14.6] for CEBPAbZIP_InDel_fs vs. 12.6 [6.2–19.1] for CEBPAbZIP_ms vs 14.6 [7.7–21.5] for CEBPAother; p < .001) and OS (median [95% CI] NA for patients with CEBPAbZIP_InDel_inf [NA–NA] vs. 25.7 months [10.2–41.3] for CEBPAbZIP_InDel_fs vs. 54.3 [14.6–NA] for CEBPAbZIP_ms vs. 45.5 [13.1–77.9] for CEBPAother; p < .001) (Figure 1B,C). Of note, a sensitivity analysis in which survival times were censored at the date of HCT in CR1 revealed almost identical results (Supporting Information S1: Figure 3).
Multivariate Cox models for EFS and OS adjusted for sex, type of AML, FLT3-ITD, NPM1 mutation status, white blood cell (WBC) count (log10 transformed), bone marrow blasts, and age including HCT in CR1 as a time-dependent variable (Supporting Information S1: Appendix) revealed increasing age and higher WBC as unfavorable factors, whereas CEBPAbZIP_InDel_inf, NPM1mut, and HCT in CR1 were favorable (Table 1).
A recent meta-analysis of 1010 adult CEBPAmut AML from six different study groups characterized CEBPA mutational subgroups in more detail by evaluating their clinical and genetic features as well as their prognostic impact.14 In line with our data, the authors showed that CEBPAbZIP_InDel_inf mutations represent a subset of AML with distinct disease biology and clinical outcomes. Despite certain limitations, in particular, the retrospective nature spanning almost three decades with evolving different treatment approaches, both studies independently confirm the less favorable impact of in-frame bZIP missense mutations (currently subsumed in the category AML with CEBPAbZIP_inf in the ICC and ELN risk classification). The less favorable impact of bZIP missense mutations might be explained by the finding that bZIP missense mutations localize differently and therefore have diverse functional consequences. CEBPAbZIP_InDel_inf predominantly affects the fork region of bZIP, while CEBPAbZIP_ms cluster in the basic region (Supporting Information S1: Figure 4). These different mutation patterns imply that CEBPAbZIP_ms impair DNA binding, while CEBPAbZIP_InDel_inf affects dimerization. Murine data have shown that missense mutations in the basic region of bZIP lead to a myeloproliferative disease transforming into overt AML,7 while AML arises upon transplantation of transgenic cells carrying the most common in-frame insertion in bZIP (K313dup, K-allele) alone or in combination with an N-terminal mutation (L-allele), with the K/L combination driving the most aggressive AML.15
In this retrospective, exploratory analysis of 528 adult patients with newly diagnosed intensively treated patients with CEBPAmut AML, we further refined the prognostic impact of different CEBPA mutation types, in particular, CEBPA mutations that are located in the bZIP domain. Our study shows that the beneficial effect is restricted to CEBPA bZIP InDel in-frame mutations, irrespective of the allelic status, whereas CEBPA bZIP missense mutations are associated with inferior outcomes. Our data as well as the data from Georgi et al. provide novel and clinically relevant results contributing to a further refinement of CEBPAmut AML in the current ICC and WHO classifications as well as for risk stratification as recommended by the ELN.
Frank G. Rücker, Andrea Corbacioglu, Hartmut Döhner, and Konstanze Döhner designed the study. Frank G. Rücker, Andrea Corbacioglu, Sibylle Cocciardi, Verena I. Gaidzik, Annika Meid, and Sophia Aicher performed experiments and validated data. Frank G. Rücker, Julia Krzykalla, Daniela Weber, and Axel Benner performed statistical analyses. Frank G. Rücker, Andrea Corbacioglu, Julia Krzykalla, Daniela Weber, Axel Benner, Hartmut Döhner, and Konstanze Döhner analyzed the results. Claudia Lengerke, Ulrich Germing, Gerald Wulf, Maisun A. Samra, Lino L. Teichmann, Michael Lübbert, Michael W. M. Kühn, Martin Bentz, Jörg Westermann, Lars Bullinger, Frank Stegelmann, Anika Schrade, Felicitas Thol, Michael Heuser, and Arnold Ganser collected and provided patient samples and clinical information. Frank G. Rücker, Andrea Corbacioglu, Hartmut Döhner, and Konstanze Döhner wrote the first draft of the manuscript; and all authors undertook manuscript writing, editing, and approval, revised the manuscript, and reviewed and approved the final version.
Frank G. Rücker reports honoraria from and consultancy for Jazz Pharmaceuticals, Novartis, and BMS/Celgene; travel support from Jazz Pharmaceuticals. Michael Lübbert reports an advisory role for Abbvie, Astex Pharmaceuticals, Imago BioSciences, Janssen, Otsuka, and Syros; research support from Janssen and Cheplapharm. Michael W. M. Kühn reports honoraria from and consultancy for Pfizer, Kura Oncology, Jazz Pharmaceuticals, BMS/Celgene, and Abbvie; speakers bureau of Gilead. Lars Bullinger reports honoraria from Abbvie, Amgen, Astellas, BMS/Celgene, Daiichi Sankyo, Gilead, Janssen, Jazz Pharmaceuticals, Menarini, Novartis, Pfizer, Roche, and Sanofi; research support from Bayer and Jazz Pharmaceuticals. Verena I. Gaidzik reports an advisory role for Jazz Pharmaceuticals, Abbvie, and Boehringer-Ingelheim; speakers bureau of Pfizer, Janssen, and Abbvie; and travel support from Abbvie. Frank Stegelmann reports honoraria from and consultancy for AOP Pharma, MorphoSys, BMS/Celgene, Incyte, Novartis, and Pfizer. Felicitas Thol reports an advisory role for Novartis, BMS, Abbvie, Menarini, and Rigel. Michael Heuser reports honoraria from Certara, Jazz Pharmaceuticals, Janssen, Novartis, and Sobi; paid consultancy for Abbvie, Amgen, BMS/Celgene, Glycostem, LabDelbert, Pfizer, PinotBio, and Servier; and research funding to his institution from Abbvie, Agios, Astellas, BMS/Celgene, Glycostem, Jazz Pharmaceuticals, Karyopharm, Loxo Oncology, and PinotBio. Hartmut Döhner declares being in an advisory role for Abbvie, Agios, Amgen, Astellas, AstraZeneca, Berlin Chemie, BMS/Celgene, Daiichi Sankyo, GEMoaB, Gilead, Janssen, Jazz Pharmaceuticals, Novartis, Servier, Stemline, and Syndax; research funding from Abbvie, Agios, Amgen, Astellas, BMS/Celgene, Jazz Pharmaceuticals, Kronos Bio, Novartis, and Pfizer. Konstanze Döhner reports an advisory role for Amgen, BMS/Celgene, Daiichi Sankyo, Janssen, Jazz Pharmaceuticals, Novartis, and Roche; research funding from Agios, Astex, Astellas, BMS/Celgene, and Novartis. All other authors declare no competing interest. The remaining authors declared no conflicts of interest.
This work was supported in part by Collaborative Research Center SFB 1074, projects B3 and B12 (K.D.) and project Z1 (H.D.).
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


