{"title":"Pain management inequities by demographic and geriatric-related variables in older adult inpatients","authors":"Aksharananda Rambachan MD, MPH, Torsten B. Neilands PhD, Leah Karliner MD, MAS, Kenneth Covinsky MD, MPH, Margaret Fang MD, MPH, Tung Nguyen MD","doi":"10.1111/jgs.19076","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Pain is ubiquitous, yet understudied. The objective of this study was to analyze inequities in pain assessment and management for hospitalized older adults focusing on demographic and geriatric-related variables.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a retrospective cohort study from January 2013 through September 2021 of all adults 65 years or older on the general medicine service at UCSF Medical Center. Primary exposures included (1) demographic variables including race/ethnicity and limited English proficiency (LEP) status and (2) geriatric-related variables including age, dementia or mild cognitive impairment diagnosis, hearing or visual impairment, end-of-life care, and geriatrics consult involvement. Primary outcomes included (1) adjusted odds of numeric pain assessment versus other assessments and (2) adjusted opioids administered, measured by morphine milligram equivalents (MME).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 15,809 patients were included across 27,857 hospitalizations with 1,378,215 pain assessments, with a mean age of 77.8 years old. Patients were 47.4% White, 26.3% with LEP, 49.6% male, and 50.4% female. Asian (OR 0.75, 95% CI 0.70–0.80), Latinx (OR 0.90, 95% CI 0.83–0.99), and Native Hawaiian or Pacific Islander (OR 0.77, 95% CI 0.64–0.93) patients had lower odds of a numeric assessment, compared with White patients. Patients with LEP (OR 0.70, 95% CI 0.66–0.74) had lower odds of a numeric assessment, compared with English-speaking patients. Patients with dementia, hearing impairment, patients 75+, and at end-of-life were all less likely to receive a numeric assessment. Compared with White patients (86 MME, 95% CI 77–96), Asian patients (55 MME, 95% CI 46–65) received fewer opioids. Patients with LEP, dementia, hearing impairment and those 75+ years old also received significantly fewer opioids.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Older, hospitalized, general medicine patients from minoritized groups and with geriatric-related conditions are uniquely vulnerable to inequitable pain assessment and management. These findings raise concerns for pain underassessment and undertreatment.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 10","pages":"3000-3010"},"PeriodicalIF":4.3000,"publicationDate":"2024-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19076","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19076","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Pain is ubiquitous, yet understudied. The objective of this study was to analyze inequities in pain assessment and management for hospitalized older adults focusing on demographic and geriatric-related variables.
Methods
This was a retrospective cohort study from January 2013 through September 2021 of all adults 65 years or older on the general medicine service at UCSF Medical Center. Primary exposures included (1) demographic variables including race/ethnicity and limited English proficiency (LEP) status and (2) geriatric-related variables including age, dementia or mild cognitive impairment diagnosis, hearing or visual impairment, end-of-life care, and geriatrics consult involvement. Primary outcomes included (1) adjusted odds of numeric pain assessment versus other assessments and (2) adjusted opioids administered, measured by morphine milligram equivalents (MME).
Results
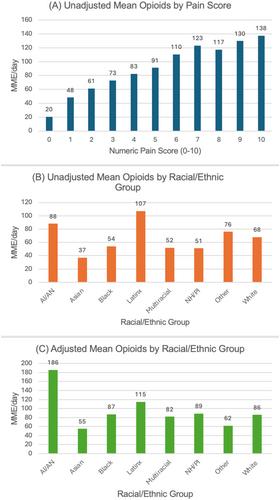
A total of 15,809 patients were included across 27,857 hospitalizations with 1,378,215 pain assessments, with a mean age of 77.8 years old. Patients were 47.4% White, 26.3% with LEP, 49.6% male, and 50.4% female. Asian (OR 0.75, 95% CI 0.70–0.80), Latinx (OR 0.90, 95% CI 0.83–0.99), and Native Hawaiian or Pacific Islander (OR 0.77, 95% CI 0.64–0.93) patients had lower odds of a numeric assessment, compared with White patients. Patients with LEP (OR 0.70, 95% CI 0.66–0.74) had lower odds of a numeric assessment, compared with English-speaking patients. Patients with dementia, hearing impairment, patients 75+, and at end-of-life were all less likely to receive a numeric assessment. Compared with White patients (86 MME, 95% CI 77–96), Asian patients (55 MME, 95% CI 46–65) received fewer opioids. Patients with LEP, dementia, hearing impairment and those 75+ years old also received significantly fewer opioids.
Conclusion
Older, hospitalized, general medicine patients from minoritized groups and with geriatric-related conditions are uniquely vulnerable to inequitable pain assessment and management. These findings raise concerns for pain underassessment and undertreatment.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


