Katherine E Douglas, Miriam T Fox, Christine C Cheston, M Laxmi Behara, Kyle A Schoppel
{"title":"Improving Interpreter Access in the Pediatric Emergency Department: A Quality Improvement Initiative.","authors":"Katherine E Douglas, Miriam T Fox, Christine C Cheston, M Laxmi Behara, Kyle A Schoppel","doi":"10.1097/pq9.0000000000000748","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An increasing proportion of the population in the United States have limited English proficiency (LEP). Hospitals that receive federal funding must offer interpreter services. However, access is often lacking for patients. Patients with LEP are at higher risk for adverse events, and the Emergency Department is a particularly high-risk environment for these events.</p><p><strong>Methods: </strong>This quality improvement initiative took place from April 2021 to August 2022 in an urban, tertiary care Pediatric Emergency Department. A driver diagram informed four Plan-Do-Study-Act cycles, and data were collected through medical record review, patient surveys, and staff surveys. We tracked outcomes using run and control chart data.</p><p><strong>Results: </strong>During the study period, the proportion of patients with LEP reporting \"always\" having an interpreter was unchanged (no centerline shift-control chart rules). Documentation of interpreter use for encounters with patients with LEP improved. Preferred language documentation and documentation of the need for an interpreter in the electronic medical record showed no change. Process measure data for staff-reported use of professional interpreters significantly increased, and the use of ad hoc interpreters decreased significantly. Length of stay did not change for English or LEP patients.</p><p><strong>Conclusions: </strong>This quality improvement initiative improved appropriate documentation of LEP and decreased use of nonqualified interpreters, although no change occurred in the proportion of patients who reported always having an interpreter. Patient satisfaction was unaffected.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 4","pages":"e748"},"PeriodicalIF":1.1000,"publicationDate":"2024-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11236402/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000748","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: An increasing proportion of the population in the United States have limited English proficiency (LEP). Hospitals that receive federal funding must offer interpreter services. However, access is often lacking for patients. Patients with LEP are at higher risk for adverse events, and the Emergency Department is a particularly high-risk environment for these events.
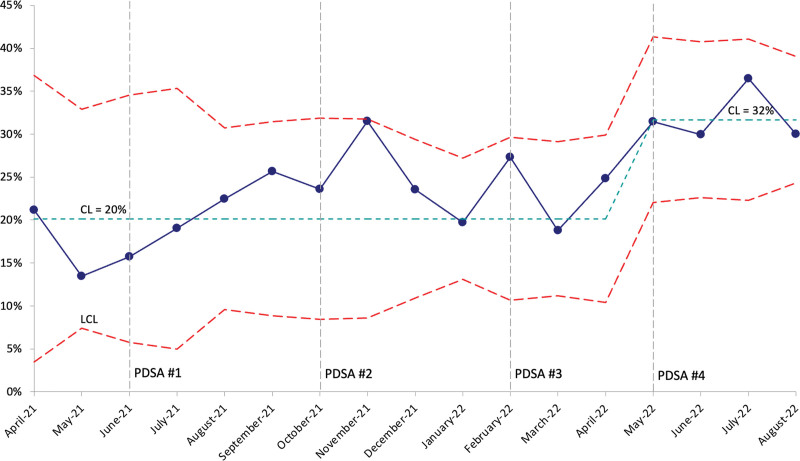
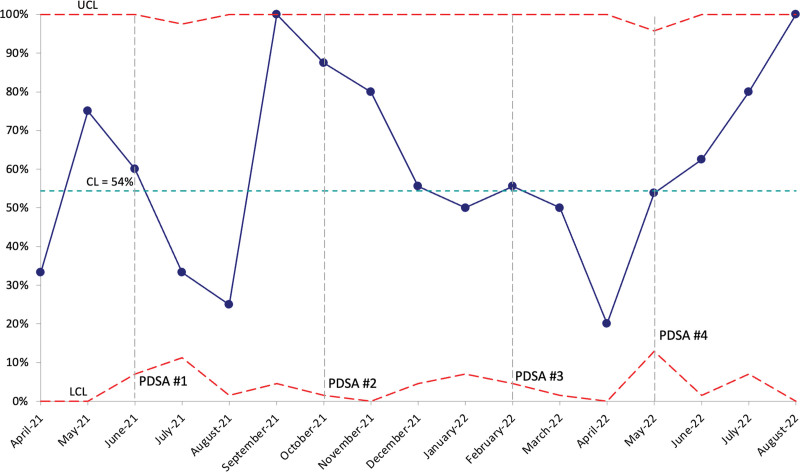
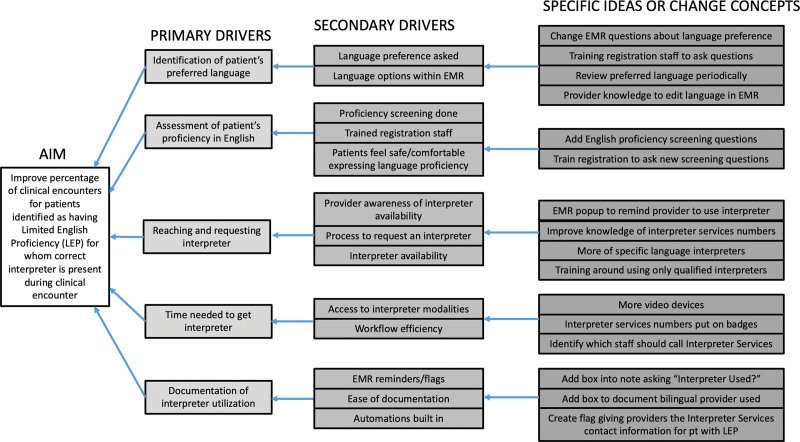
Methods: This quality improvement initiative took place from April 2021 to August 2022 in an urban, tertiary care Pediatric Emergency Department. A driver diagram informed four Plan-Do-Study-Act cycles, and data were collected through medical record review, patient surveys, and staff surveys. We tracked outcomes using run and control chart data.
Results: During the study period, the proportion of patients with LEP reporting "always" having an interpreter was unchanged (no centerline shift-control chart rules). Documentation of interpreter use for encounters with patients with LEP improved. Preferred language documentation and documentation of the need for an interpreter in the electronic medical record showed no change. Process measure data for staff-reported use of professional interpreters significantly increased, and the use of ad hoc interpreters decreased significantly. Length of stay did not change for English or LEP patients.
Conclusions: This quality improvement initiative improved appropriate documentation of LEP and decreased use of nonqualified interpreters, although no change occurred in the proportion of patients who reported always having an interpreter. Patient satisfaction was unaffected.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


