{"title":"Adipsic hypernatremia with marked hyperprolactinemia and GH deficiency in a 9-year-old boy.","authors":"Hisato Segoe, Akie Nakamura, Kimiaki Uetake, Nozomi Hishimura, Naoya Kaneko, Shuntaro Morikawa, Akari Nakamura-Utsunomiya, Takeshi Yamaguchi","doi":"10.1297/cpe.2024-0001","DOIUrl":null,"url":null,"abstract":"<p><p>Adipsic hypernatremia is typically caused by congenital dysplasia of the hypothalamus and pituitary or brain tumors. However, cases of adipsic hypernatremia without underlying organic abnormalities are rare, and some cases have been reported to be complicated by hypothalamic-pituitary dysfunction. The patient in this case was a 9-yr-old boy who was referred to our hospital because of hypernatremia. His growth chart revealed that he had rapidly become obese since infancy, with growth retardation since the age of seven. His hands and feet were very cold, and he had erythema on his abdomen, indicating possible autonomic dysregulation due to hypothalamic dysfunction. Several hormone load tests showed severe GH deficiency (GHD) and marked hyperprolactinemia (peak: 302.8 ng/mL). Magnetic resonance imaging revealed no organic abnormalities in the hypothalamus and pituitary gland. GH replacement therapy was initiated. Although his growth rate improved, obesity persisted. To the best of our knowledge, this is the first report of adipsic hypernatremia without organic intracranial abnormalities that was treated with GH. Moreover, the patient's prolactin levels were higher than those reported in previous studies. In conclusion, adipsic hypernatremia requires the evaluation of pituitary function and appropriate therapeutic interventions.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":"33 3","pages":"163-168"},"PeriodicalIF":1.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11234189/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2024-0001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/22 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
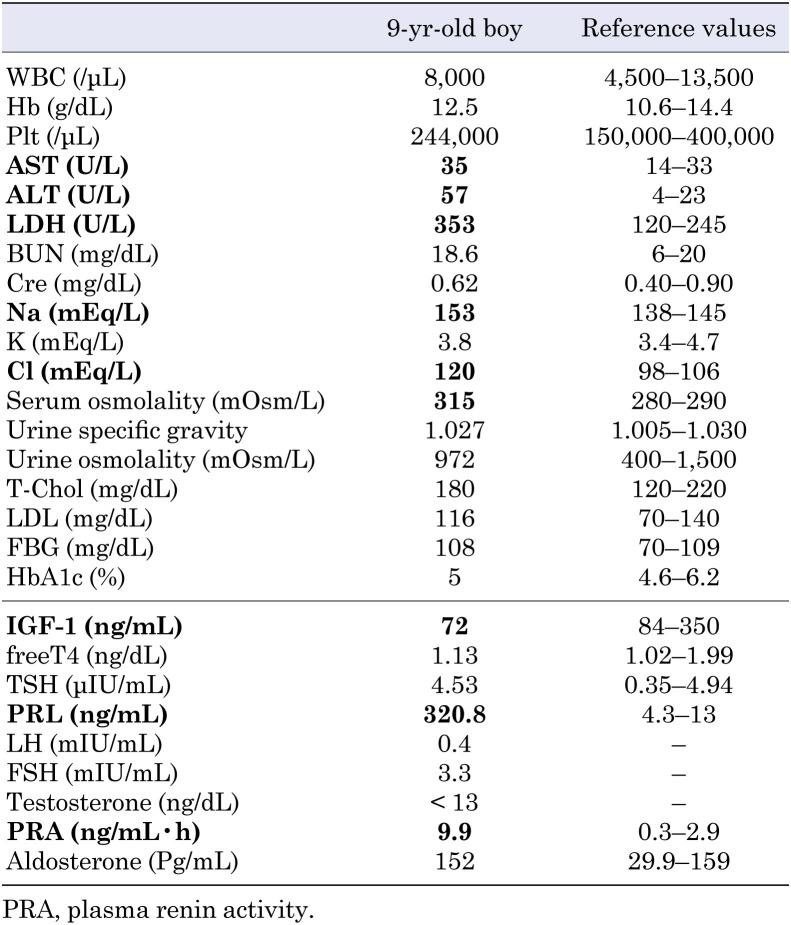
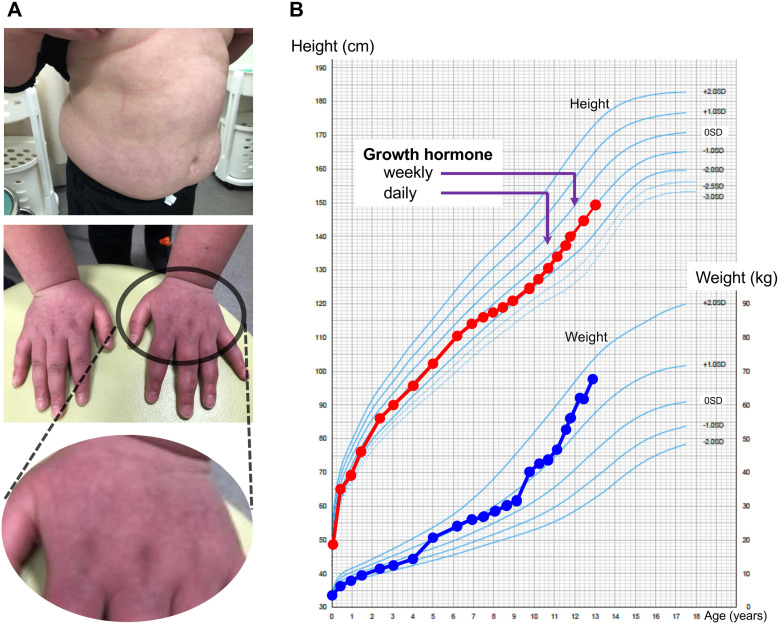
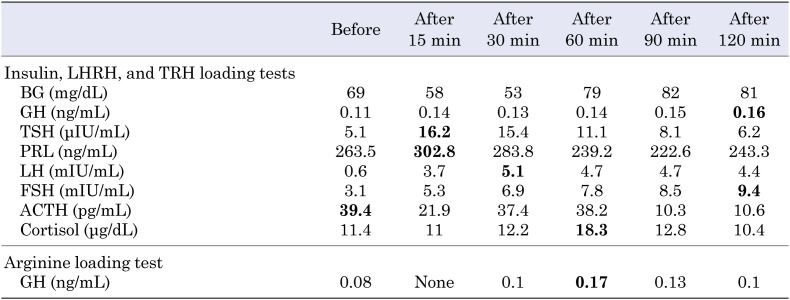
Adipsic hypernatremia is typically caused by congenital dysplasia of the hypothalamus and pituitary or brain tumors. However, cases of adipsic hypernatremia without underlying organic abnormalities are rare, and some cases have been reported to be complicated by hypothalamic-pituitary dysfunction. The patient in this case was a 9-yr-old boy who was referred to our hospital because of hypernatremia. His growth chart revealed that he had rapidly become obese since infancy, with growth retardation since the age of seven. His hands and feet were very cold, and he had erythema on his abdomen, indicating possible autonomic dysregulation due to hypothalamic dysfunction. Several hormone load tests showed severe GH deficiency (GHD) and marked hyperprolactinemia (peak: 302.8 ng/mL). Magnetic resonance imaging revealed no organic abnormalities in the hypothalamus and pituitary gland. GH replacement therapy was initiated. Although his growth rate improved, obesity persisted. To the best of our knowledge, this is the first report of adipsic hypernatremia without organic intracranial abnormalities that was treated with GH. Moreover, the patient's prolactin levels were higher than those reported in previous studies. In conclusion, adipsic hypernatremia requires the evaluation of pituitary function and appropriate therapeutic interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


