Bülent Zülfikar, Johnny Mahlangu, Salim Mohamed Nekkal, Cecil Ross, Noppacharn Uaprasert, Jerzy Windyga, Carmen Escuriola Ettingshausen, Bettina Ploder, Aurelia Lelli, Hanna T Gazda
{"title":"Reduced Volume and Faster Infusion Rate of Activated Prothrombin Complex Concentrate: A Phase 3b/4 Trial in Adults with Hemophilia A with Inhibitors.","authors":"Bülent Zülfikar, Johnny Mahlangu, Salim Mohamed Nekkal, Cecil Ross, Noppacharn Uaprasert, Jerzy Windyga, Carmen Escuriola Ettingshausen, Bettina Ploder, Aurelia Lelli, Hanna T Gazda","doi":"10.1055/s-0044-1787781","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Activated prothrombin complex concentrate (aPCC) is indicated for bleed treatment and prevention in patients with hemophilia with inhibitors. The safety and tolerability of intravenous aPCC at a reduced volume and faster infusion rates were evaluated. <b>Methods</b> This multicenter, open-label trial (NCT02764489) enrolled adults with hemophilia A with inhibitors. In part 1, patients were randomized to receive three infusions of aPCC (85 ± 15 U/kg) at 2 U/kg/min (the approved standard rate at the time of the study), in a regular or 50% reduced volume, and were then crossed over to receive three infusions in the alternative volume. In part 2, patients received three sequential infusions of aPCC in a 50% reduced volume at 4 U/kg/min and then at 10 U/kg/min. Primary outcome measures included the incidence of adverse events (AEs), allergic-type hypersensitivity reactions (AHRs), infusion-site reactions (ISRs), and thromboembolic events. <b>Results</b> Of the 45 patients enrolled, 33 received aPCC in part 1 and 30 in part 2. In part 1, 24.2 and 23.3% of patients with regular and reduced volumes experienced AEs, respectively; 11 AEs in eight patients were treatment related. AHRs and ISRs occurred in four (12.1%) and two (6.1%) patients, respectively. In part 2, 3.3 and 14.3% of patients with infusion rates of 4 and 10 U/kg/min experienced AEs, respectively; only one AE in one patient was treatment related; no AHRs or ISRs were reported. Most AEs were mild/moderate in severity. Overall, no thromboembolic events were reported. <b>Conclusions</b> aPCC was well tolerated at a reduced volume and faster infusion rates, with safety profiles comparable to the approved regimen.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"8 3","pages":"e273-e282"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11230701/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1787781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
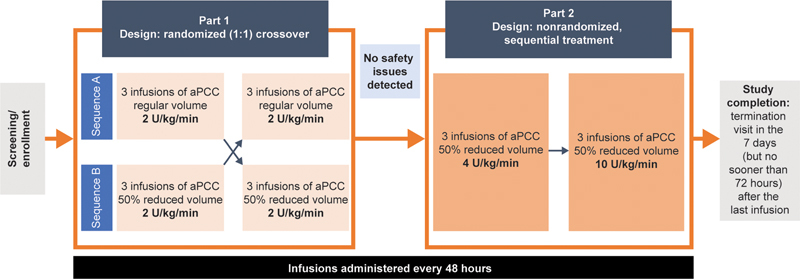
Background Activated prothrombin complex concentrate (aPCC) is indicated for bleed treatment and prevention in patients with hemophilia with inhibitors. The safety and tolerability of intravenous aPCC at a reduced volume and faster infusion rates were evaluated. Methods This multicenter, open-label trial (NCT02764489) enrolled adults with hemophilia A with inhibitors. In part 1, patients were randomized to receive three infusions of aPCC (85 ± 15 U/kg) at 2 U/kg/min (the approved standard rate at the time of the study), in a regular or 50% reduced volume, and were then crossed over to receive three infusions in the alternative volume. In part 2, patients received three sequential infusions of aPCC in a 50% reduced volume at 4 U/kg/min and then at 10 U/kg/min. Primary outcome measures included the incidence of adverse events (AEs), allergic-type hypersensitivity reactions (AHRs), infusion-site reactions (ISRs), and thromboembolic events. Results Of the 45 patients enrolled, 33 received aPCC in part 1 and 30 in part 2. In part 1, 24.2 and 23.3% of patients with regular and reduced volumes experienced AEs, respectively; 11 AEs in eight patients were treatment related. AHRs and ISRs occurred in four (12.1%) and two (6.1%) patients, respectively. In part 2, 3.3 and 14.3% of patients with infusion rates of 4 and 10 U/kg/min experienced AEs, respectively; only one AE in one patient was treatment related; no AHRs or ISRs were reported. Most AEs were mild/moderate in severity. Overall, no thromboembolic events were reported. Conclusions aPCC was well tolerated at a reduced volume and faster infusion rates, with safety profiles comparable to the approved regimen.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


