{"title":"The Global Burden of Resistant Hypertension and Potential Treatment Options.","authors":"Giacomo Buso, Claudia Agabiti-Rosei, Matteo Lemoli, Federica Corvini, Maria Lorenza Muiesan","doi":"10.15420/ecr.2023.51","DOIUrl":null,"url":null,"abstract":"<p><p>Resistant hypertension (RH) is defined as systolic blood pressure (SBP) or diastolic blood pressure (DBP) that remains .140 mmHg or .90 mmHg, respectively, despite an appropriate lifestyle and the use of optimal or maximally tolerated doses of a three-drug combination, including a diuretic. This definition encompasses the category of controlled RH, defined as the presence of blood pressure (BP) effectively controlled by four or more antihypertensive agents, as well as refractory hypertension, referred to as uncontrolled BP despite five or more drugs of different classes, including a diuretic. To confirm RH presence, various causes of pseudo-resistant hypertension (such as improper BP measurement techniques and poor medication adherence) and secondary hypertension must be ruled out. Inadequate BP control should be confirmed by out-of-office BP measurement. RH affects about 5% of the hypertensive population and is associated with increased cardiovascular morbidity and mortality. Once RH presence is confirmed, patient evaluation includes identification of contributing factors such as lifestyle issues or interfering drugs/substances and assessment of hypertension-mediated organ damage. Management of RH comprises lifestyle interventions and optimisation of current medication therapy. Additional drugs should be introduced sequentially if BP remains uncontrolled and renal denervation can be considered as an additional treatment option. However, achieving optimal BP control remains challenging in this setting. This review aims to provide an overview of RH, including its epidemiology, pathophysiology, diagnostic work-up, as well as the latest therapeutic developments.</p>","PeriodicalId":93994,"journal":{"name":"European cardiology","volume":"19 ","pages":"e07"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11231817/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/ecr.2023.51","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
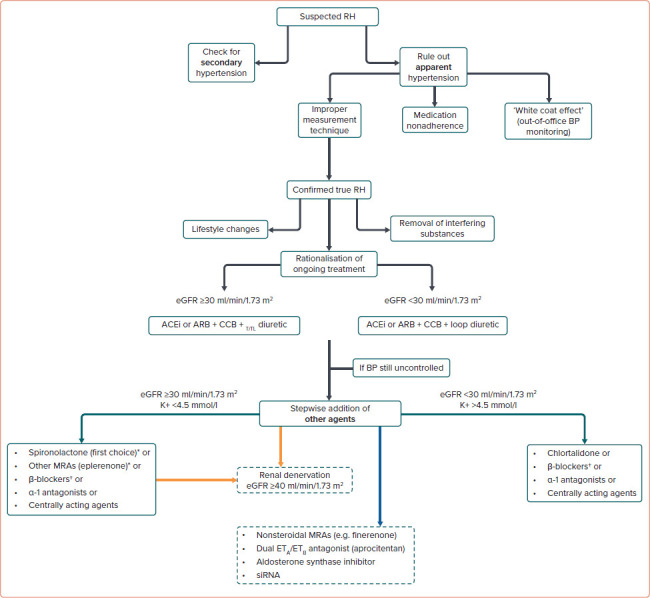
Resistant hypertension (RH) is defined as systolic blood pressure (SBP) or diastolic blood pressure (DBP) that remains .140 mmHg or .90 mmHg, respectively, despite an appropriate lifestyle and the use of optimal or maximally tolerated doses of a three-drug combination, including a diuretic. This definition encompasses the category of controlled RH, defined as the presence of blood pressure (BP) effectively controlled by four or more antihypertensive agents, as well as refractory hypertension, referred to as uncontrolled BP despite five or more drugs of different classes, including a diuretic. To confirm RH presence, various causes of pseudo-resistant hypertension (such as improper BP measurement techniques and poor medication adherence) and secondary hypertension must be ruled out. Inadequate BP control should be confirmed by out-of-office BP measurement. RH affects about 5% of the hypertensive population and is associated with increased cardiovascular morbidity and mortality. Once RH presence is confirmed, patient evaluation includes identification of contributing factors such as lifestyle issues or interfering drugs/substances and assessment of hypertension-mediated organ damage. Management of RH comprises lifestyle interventions and optimisation of current medication therapy. Additional drugs should be introduced sequentially if BP remains uncontrolled and renal denervation can be considered as an additional treatment option. However, achieving optimal BP control remains challenging in this setting. This review aims to provide an overview of RH, including its epidemiology, pathophysiology, diagnostic work-up, as well as the latest therapeutic developments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


