Christine Hakimeh, Kourosh Shahraki, Luc Courtois, Donny W Suh
{"title":"Surgical management of chronic sixth cranial nerve palsy: case report and literature review.","authors":"Christine Hakimeh, Kourosh Shahraki, Luc Courtois, Donny W Suh","doi":"10.51329/mehdiophthal1494","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Esotropia resulting from sixth cranial nerve palsy can substantially impact an individual's visual acuity and overall quality of life. If the condition does not resolve in 6-10 months, surgical intervention may be necessary. Various muscle surgeries may be considered, with vertical rectus muscle transposition emerging as the primary option for treatment of complete palsy. However, this technique carries the risk of anterior segment ischemia and post-surgery deviations. Herein, we present a successful treatment of chronic complete sixth nerve palsy using a modified Nishida procedure, without splitting or tenotomy, and an adjunct botulinum toxin A (BTA) injection in the ipsilateral medial rectus muscle.</p><p><strong>Case presentation: </strong>A 59-year-old woman with a history of traumatic sixth nerve palsy had previously undergone horizontal muscle strabismus surgeries. Following multiple left medial rectus recessions, lateral rectus resection, and BTA injections, esotropia persisted. The worsening of her condition led to emotional distress and impaired social interaction. Initial examination revealed marked esotropia and limited left eye abduction. Magnetic resonance imaging (SIGNA MR750w, GE Healthcare, Waukesha, WI, USA) of the left eye revealed a contracted medial rectus muscle and substantial atrophy of the left lateral rectus muscle. A modified Nishida procedure was performed with an injection of 3 units of BTA into the ipsilateral medial rectus muscle, resulting in improved ocular alignment and stable findings after nine postoperative months. Furthermore, we supported our successful outcome with a summary of similar reported cases of sixth nerve palsy managed using the modified Nishida procedure with or without adjunctive procedures.</p><p><strong>Conclusions: </strong>Following the modified Nishida procedure, the patient experienced a reduction in diplopia, improved ocular alignment and stability, and an increased binocular diplopia-free field. This case underscores the importance of an individualized approach to complex strabismus cases and highlights the modified Nishida procedure as a valuable tool in such circumstances. In the future, strabismus management will focus on refining personalized treatment and exploring innovative techniques for complex cases. Our success in using a combination of Nishida procedure and BTA injection should be further investigated in large-scale studies.</p>","PeriodicalId":36524,"journal":{"name":"Medical Hypothesis, Discovery, and Innovation in Ophthalmology","volume":"13 1","pages":"55-62"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11227665/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Hypothesis, Discovery, and Innovation in Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.51329/mehdiophthal1494","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Esotropia resulting from sixth cranial nerve palsy can substantially impact an individual's visual acuity and overall quality of life. If the condition does not resolve in 6-10 months, surgical intervention may be necessary. Various muscle surgeries may be considered, with vertical rectus muscle transposition emerging as the primary option for treatment of complete palsy. However, this technique carries the risk of anterior segment ischemia and post-surgery deviations. Herein, we present a successful treatment of chronic complete sixth nerve palsy using a modified Nishida procedure, without splitting or tenotomy, and an adjunct botulinum toxin A (BTA) injection in the ipsilateral medial rectus muscle.
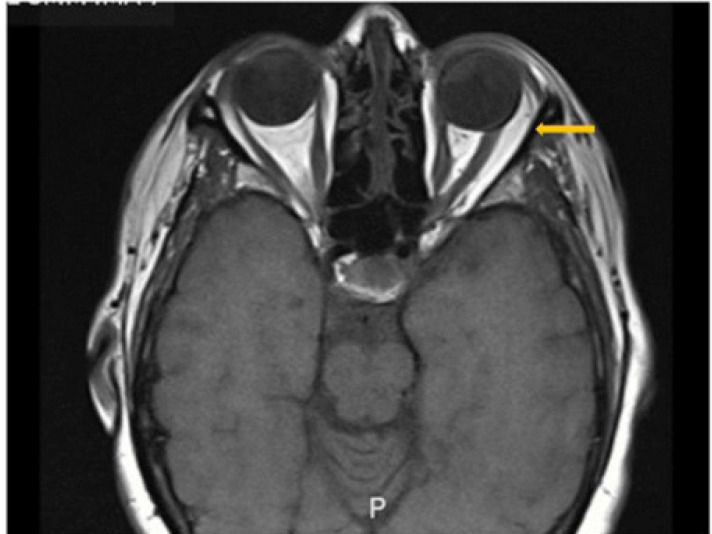
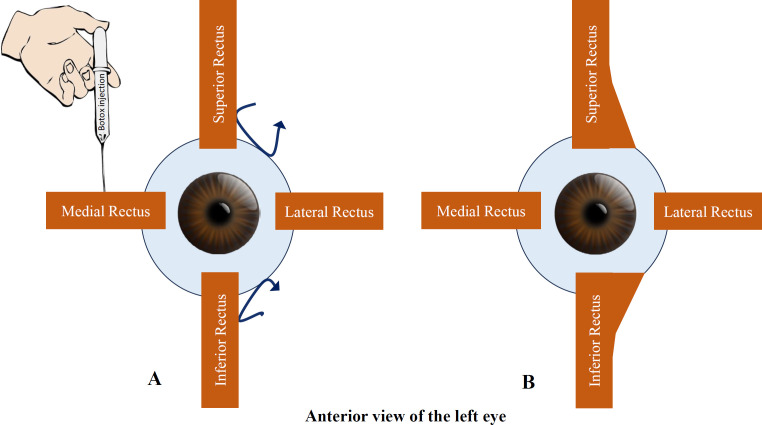
Case presentation: A 59-year-old woman with a history of traumatic sixth nerve palsy had previously undergone horizontal muscle strabismus surgeries. Following multiple left medial rectus recessions, lateral rectus resection, and BTA injections, esotropia persisted. The worsening of her condition led to emotional distress and impaired social interaction. Initial examination revealed marked esotropia and limited left eye abduction. Magnetic resonance imaging (SIGNA MR750w, GE Healthcare, Waukesha, WI, USA) of the left eye revealed a contracted medial rectus muscle and substantial atrophy of the left lateral rectus muscle. A modified Nishida procedure was performed with an injection of 3 units of BTA into the ipsilateral medial rectus muscle, resulting in improved ocular alignment and stable findings after nine postoperative months. Furthermore, we supported our successful outcome with a summary of similar reported cases of sixth nerve palsy managed using the modified Nishida procedure with or without adjunctive procedures.
Conclusions: Following the modified Nishida procedure, the patient experienced a reduction in diplopia, improved ocular alignment and stability, and an increased binocular diplopia-free field. This case underscores the importance of an individualized approach to complex strabismus cases and highlights the modified Nishida procedure as a valuable tool in such circumstances. In the future, strabismus management will focus on refining personalized treatment and exploring innovative techniques for complex cases. Our success in using a combination of Nishida procedure and BTA injection should be further investigated in large-scale studies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


