Helen Ullrich-Daub, Maximilian Olschewski, Boris Schnorbus, Khelifa-Anis Belhadj, Till Köhler, Markus Vosseler, Thomas Münzel, Tommaso Gori
{"title":"Quantitative flow ratio or angiography for the assessment of non-culprit lesions in acute coronary syndromes, a randomized trial.","authors":"Helen Ullrich-Daub, Maximilian Olschewski, Boris Schnorbus, Khelifa-Anis Belhadj, Till Köhler, Markus Vosseler, Thomas Münzel, Tommaso Gori","doi":"10.1007/s00392-024-02484-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients undergoing percutaneous coronary intervention for acute coronary syndromes often have multivessel disease (MVD). Quantitative flow ratio (QFR) is an angiography-based technology that may help quantify the functional significance of non-culprit lesions, with the advantage that measurements are possible also once the patient is discharged from the catheterization laboratory.</p><p><strong>Aim: </strong>Our two-center, randomized superiority trial aimed to test whether QFR, as compared to angiography, modifies the rate of non-culprit lesion interventions (primary functional endpoint) and improves the outcomes of patients with acute coronary syndromes and MVD (primary clinical endpoint).</p><p><strong>Methods: </strong>In total, 202 consecutive patients (64 [56-71] years of age, 160 men) with STEMI (n = 69 (34%)), NSTEMI (n = 94 (47%)), or unstable angina (n = 39 (19%)) and MVD who had undergone successful treatment of all culprit lesions were randomized 1:1 to angiography- vs. QFR-guided delayed revascularization of 246 non-culprit stenoses (1.2/patient).</p><p><strong>Results: </strong>The proportion of patients assigned to percutaneous intervention was not different between groups (angiography group: 45 (45%) vs. QFR: 56 (55%), P = 0.125; relative risk = 0.80 (0.60-1.06)). At 12 months, a primary clinical endpoint event (composite of death, nonfatal myocardial infarction, revascularization, and significant angina) occurred in 24 patients (angiography-guided) and 23 patients (QFR-guided; P = 0.637, HR = 1.16 [0.63-2.15]). None of its components was different between groups.</p><p><strong>Discussion: </strong>QFR guidance based on analysis of images from the primary intervention was not associated with a difference in the rate of non-culprit lesion staged revascularization nor in the 12-month incidence of clinical events in patients with acute coronary syndromes and multivessel disease.</p><p><strong>Trial registration number: </strong>ClinicalTrials.gov Registry (NCT04808310).</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"729-737"},"PeriodicalIF":3.8000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12089241/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02484-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients undergoing percutaneous coronary intervention for acute coronary syndromes often have multivessel disease (MVD). Quantitative flow ratio (QFR) is an angiography-based technology that may help quantify the functional significance of non-culprit lesions, with the advantage that measurements are possible also once the patient is discharged from the catheterization laboratory.
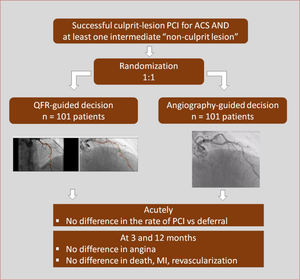
Aim: Our two-center, randomized superiority trial aimed to test whether QFR, as compared to angiography, modifies the rate of non-culprit lesion interventions (primary functional endpoint) and improves the outcomes of patients with acute coronary syndromes and MVD (primary clinical endpoint).
Methods: In total, 202 consecutive patients (64 [56-71] years of age, 160 men) with STEMI (n = 69 (34%)), NSTEMI (n = 94 (47%)), or unstable angina (n = 39 (19%)) and MVD who had undergone successful treatment of all culprit lesions were randomized 1:1 to angiography- vs. QFR-guided delayed revascularization of 246 non-culprit stenoses (1.2/patient).
Results: The proportion of patients assigned to percutaneous intervention was not different between groups (angiography group: 45 (45%) vs. QFR: 56 (55%), P = 0.125; relative risk = 0.80 (0.60-1.06)). At 12 months, a primary clinical endpoint event (composite of death, nonfatal myocardial infarction, revascularization, and significant angina) occurred in 24 patients (angiography-guided) and 23 patients (QFR-guided; P = 0.637, HR = 1.16 [0.63-2.15]). None of its components was different between groups.
Discussion: QFR guidance based on analysis of images from the primary intervention was not associated with a difference in the rate of non-culprit lesion staged revascularization nor in the 12-month incidence of clinical events in patients with acute coronary syndromes and multivessel disease.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


