Blood pressure increases are associated with weight gain and not antiretroviral regimen or kidney function: a secondary analysis from the ADVANCE trial in South Africa
Abstract
Introduction
Recent evidence has raised questions about whether newer HIV treatment regimens, including dolutegravir (DTG) and tenofovir alafenamide (TAF), are associated with increases in blood pressure (BP).
Methods
We assessed changes in BP by treatment regimen and evaluated the relative contribution of kidney function and weight gain to these changes among participants in the ADVANCE phase-3 trial clinical trial in South Africa (study dates: January 2017–February 2022). Our primary outcome of interest was a change in systolic BP (SBP) at 96 and 192 weeks, among those not receiving antihypertensive medication. The secondary outcome was treatment-emergent hypertension at these same time points, defined as BP ≥140/90 mmHg on two occasions, or initiation of antihypertensive medication after week 4 among individuals without hypertension at enrolment. We used linear regression to evaluate the relationship between change in estimated glomerular filtration rate (eGFR) and change in SBP; and Poisson regression to evaluate the relationship between change in eGFR and treatment-emergent hypertension at each time point. All models were adjusted for age, sex, treatment group and change in body mass index (BMI).
Results
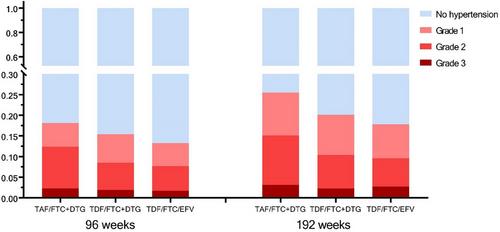
Over 96 weeks, the average changes in SBP were 1.7 mmHg (95% CI: 0.0−3.4), −0.5 mmHg (95% CI: −2.2 to 1.7) and −2.1 mmHg (95% CI: −3.8 to 0.4) in the TAF/emtricitabine (FTC)/DTG, tenofovir disoproxil fumarate (TDF)/FTC/DTG and TDF/FTC/efavirenz (EFV) groups, respectively. This difference was significant for the TAF/FTC/DTG compared to the TDF/FTC/EFV group (p = 0.002). Over 96 weeks, 18.2% (95% CI: 13.4–22.9), 15.4% (95% CI: 11.0–19.9) and 13.3% (95% CI: 8.9–17.6) of participants developed treatment-emergent hypertension, respectively. In adjusted models, there was no significant relationship between change in eGFR and either outcome. Change in BMI was significantly associated with an increase in SBP, while age was associated with an increased risk of treatment-emergent hypertension. Adjustment for BMI also mitigated the unadjusted relationship between HIV treatment regimen and SBP where present.
Conclusions
In the ADVANCE cohort, weight gain and age accounted for increases in BP and risk of treatment-emergent hypertension. HIV treatment programmes may need to integrate the management of obesity and hypertension into routine care.
Clinical Trial Number
NCT03122262

| 公司名称 | 产品信息 | 采购帮参考价格 |
|---|
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


