Ajai Chari, Jonathan L. Kaufman, Jacob Laubach, Douglas W. Sborov, Brandi Reeves, Cesar Rodriguez, Rebecca Silbermann, Luciano J. Costa, Larry D. Anderson, Nitya Nathwani, Nina Shah, Naresh Bumma, Sarah A. Holstein, Caitlin Costello, Andrzej Jakubowiak, Tanya M. Wildes, Robert Z. Orlowski, Kenneth H. Shain, Andrew J. Cowan, Huiling Pei, Annelore Cortoos, Sharmila Patel, Thomas S. Lin, Peter M. Voorhees, Saad Z. Usmani, Paul G. Richardson
{"title":"Daratumumab in transplant-eligible patients with newly diagnosed multiple myeloma: final analysis of clinically relevant subgroups in GRIFFIN","authors":"Ajai Chari, Jonathan L. Kaufman, Jacob Laubach, Douglas W. Sborov, Brandi Reeves, Cesar Rodriguez, Rebecca Silbermann, Luciano J. Costa, Larry D. Anderson, Nitya Nathwani, Nina Shah, Naresh Bumma, Sarah A. Holstein, Caitlin Costello, Andrzej Jakubowiak, Tanya M. Wildes, Robert Z. Orlowski, Kenneth H. Shain, Andrew J. Cowan, Huiling Pei, Annelore Cortoos, Sharmila Patel, Thomas S. Lin, Peter M. Voorhees, Saad Z. Usmani, Paul G. Richardson","doi":"10.1038/s41408-024-01088-6","DOIUrl":null,"url":null,"abstract":"<p>The randomized, phase 2 GRIFFIN study (NCT02874742) evaluated daratumumab plus lenalidomide/bortezomib/dexamethasone (D-RVd) in transplant-eligible newly diagnosed multiple myeloma (NDMM). We present final post hoc analyses (median follow-up, 49.6 months) of clinically relevant subgroups, including patients with high-risk cytogenetic abnormalities (HRCAs) per revised definition (del[17p], t[4;14], t[14;16], t[14;20], and/or gain/amp[1q21]). Patients received 4 induction cycles (D-RVd/RVd), high-dose therapy/transplant, 2 consolidation cycles (D-RVd/RVd), and lenalidomide±daratumumab maintenance (≤ 2 years). Minimal residual disease–negativity (10<sup>−5</sup>) rates were higher for D-RVd versus RVd in patients ≥ 65 years (67.9% vs 17.9%), with HRCAs (54.8% vs 32.4%), and with gain/amp(1q21) (61.8% vs 28.6%). D-RVd showed a trend toward improved progression-free survival versus RVd (hazard ratio [95% confidence interval]) in patients ≥ 65 years (0.29 [0.06–1.48]), with HRCAs (0.38 [0.14–1.01]), and with gain/amp(1q21) (0.42 [0.14–1.27]). In the functional high-risk subgroup (not MRD negative at the end of consolidation), the hazard ratio was 0.82 (0.35–1.89). Among patients ≥ 65 years, grade 3/4 treatment-emergent adverse event (TEAE) rates were higher for D-RVd versus RVd (88.9% vs 77.8%), as were TEAEs leading to discontinuation of ≥ 1 treatment component (37.0% vs 25.9%). One D-RVd patient died due to an unrelated TEAE. These results support the addition of daratumumab to RVd in transplant-eligible patients with high-risk NDMM.</p><figure></figure><script src=\"//e.video-cdn.net/v2/embed.js\"></script><p>Video Abstract</p>","PeriodicalId":8989,"journal":{"name":"Blood Cancer Journal","volume":"49 1","pages":""},"PeriodicalIF":12.9000,"publicationDate":"2024-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Cancer Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41408-024-01088-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
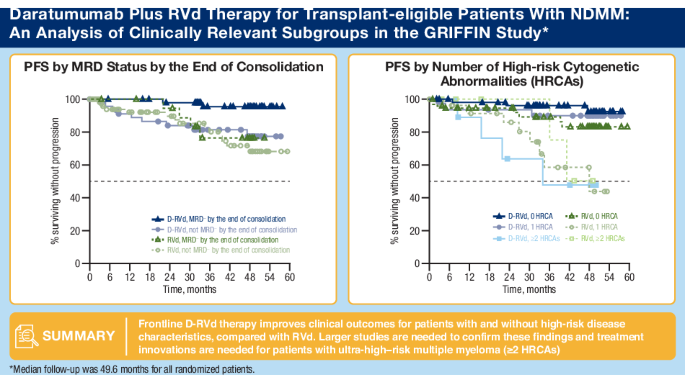
The randomized, phase 2 GRIFFIN study (NCT02874742) evaluated daratumumab plus lenalidomide/bortezomib/dexamethasone (D-RVd) in transplant-eligible newly diagnosed multiple myeloma (NDMM). We present final post hoc analyses (median follow-up, 49.6 months) of clinically relevant subgroups, including patients with high-risk cytogenetic abnormalities (HRCAs) per revised definition (del[17p], t[4;14], t[14;16], t[14;20], and/or gain/amp[1q21]). Patients received 4 induction cycles (D-RVd/RVd), high-dose therapy/transplant, 2 consolidation cycles (D-RVd/RVd), and lenalidomide±daratumumab maintenance (≤ 2 years). Minimal residual disease–negativity (10−5) rates were higher for D-RVd versus RVd in patients ≥ 65 years (67.9% vs 17.9%), with HRCAs (54.8% vs 32.4%), and with gain/amp(1q21) (61.8% vs 28.6%). D-RVd showed a trend toward improved progression-free survival versus RVd (hazard ratio [95% confidence interval]) in patients ≥ 65 years (0.29 [0.06–1.48]), with HRCAs (0.38 [0.14–1.01]), and with gain/amp(1q21) (0.42 [0.14–1.27]). In the functional high-risk subgroup (not MRD negative at the end of consolidation), the hazard ratio was 0.82 (0.35–1.89). Among patients ≥ 65 years, grade 3/4 treatment-emergent adverse event (TEAE) rates were higher for D-RVd versus RVd (88.9% vs 77.8%), as were TEAEs leading to discontinuation of ≥ 1 treatment component (37.0% vs 25.9%). One D-RVd patient died due to an unrelated TEAE. These results support the addition of daratumumab to RVd in transplant-eligible patients with high-risk NDMM.
随机2期GRIFFIN研究(NCT02874742)评估了达拉单抗联合来那度胺/硼替佐米/地塞米松(D-RVd)治疗符合移植条件的新诊断多发性骨髓瘤(NDMM)。我们对临床相关亚组进行了最终的事后分析(中位随访时间为 49.6 个月),包括根据修订后的定义(del[17p]、t[4;14]、t[14;16]、t[14;20]和/或 gain/amp[1q21])出现高危细胞遗传学异常(HRCAs)的患者。患者接受4个诱导周期(D-RVd/RVd)、大剂量治疗/移植、2个巩固周期(D-RVd/RVd)和来那度胺±达拉单抗维持治疗(≤2年)。在年龄≥65岁(67.9% vs 17.9%)、HRCAs(54.8% vs 32.4%)和增益/amp(1q21)(61.8% vs 28.6%)的患者中,D-RVd与RVd相比,最小残留病灶阴性率(10-5)更高。在年龄≥65 岁(0.29 [0.06-1.48])、患有 HRCAs(0.38 [0.14-1.01])和患有增益/amp(1q21)(0.42 [0.14-1.27])的患者中,D-RVd 与 RVd 相比显示出无进展生存期改善的趋势(危险比 [95% 置信区间])。在功能性高危亚组(巩固治疗结束时MRD未阴性)中,危险比为0.82(0.35-1.89)。在年龄≥65岁的患者中,D-RVd与RVd相比,3/4级治疗突发不良事件(TEAE)发生率更高(88.9% vs 77.8%),导致中断≥一种治疗成分的TEAE发生率也更高(37.0% vs 25.9%)。一名D-RVd患者死于与此无关的TEAE。这些结果支持在符合移植条件的高危NDMM患者中将达拉单抗加入RVd。
期刊介绍:
Blood Cancer Journal is dedicated to publishing high-quality articles related to hematologic malignancies and related disorders. The journal welcomes submissions of original research, reviews, guidelines, and letters that are deemed to have a significant impact in the field. While the journal covers a wide range of topics, it particularly focuses on areas such as:
Preclinical studies of new compounds, especially those that provide mechanistic insights
Clinical trials and observations
Reviews related to new drugs and current management of hematologic malignancies
Novel observations related to new mutations, molecular pathways, and tumor genomics
Blood Cancer Journal offers a forum for expedited publication of novel observations regarding new mutations or altered pathways.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


