Determinants of prehospital and in-hospital delay in patients with symptomatic carotid stenosis and their influence on the outcome after elective carotid endarterectomy.
Felix Kirchhoff, Christoph Knappich, Michael Kallmayer, Bianca Bohmann, Vanessa Lohe, Pavlos Tsantilas, Shamsun Naher, Hans-Henning Eckstein, Andreas Kühnl
{"title":"Determinants of prehospital and in-hospital delay in patients with symptomatic carotid stenosis and their influence on the outcome after elective carotid endarterectomy.","authors":"Felix Kirchhoff, Christoph Knappich, Michael Kallmayer, Bianca Bohmann, Vanessa Lohe, Pavlos Tsantilas, Shamsun Naher, Hans-Henning Eckstein, Andreas Kühnl","doi":"10.1136/svn-2024-003098","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study analyses the determinants of prehospital (index event to admission) and in-hospital delay (admission to carotid endarterectomy (CEA)). In addition, the analysis addresses the association between prehospital or in-hospital delay and outcomes after CEA for symptomatic patients in German hospitals.</p><p><strong>Materials and methods: </strong>This retrospective analysis is based on the nationwide German statutory quality assurance database. 55 437 patients were included in the analysis. Prehospital delay was grouped as follows: 180-15, 14-8, 7-3, 2-0 days or 'in-hospital index event'. In-hospital delay was divided into: 0-1, 2-3 and >3 days. The primary outcome event (POE) was in-hospital stroke or death. Univariate and multivariable regression analyses were performed for statistical analysis. The slope of the linear regression line is given as the β-value, and the rate parameter of the logistic regression is given as the adjusted OR (aOR).</p><p><strong>Results: </strong>Prehospital delay was 0-2 days in 34.9%, 3-14 days in 29.5% and >14 days in 18.6%. Higher age (β=-1.08, p<0.001) and a more severe index event (transitory ischaemic attack: β=-4.41, p<0.001; stroke: β=-6.05, p<0.001, Ref: amaurosis fugax) were determinants of shorter prehospital delay. Higher age (β=0.28, p<0.001) and female sex (β=0.09, p=0.014) were associated with a longer in-hospital delay. Index event after admission (aOR 1.23, 95% CI: 1.04 to 1.47) and an intermediate in-hospital delay of 2-3 days (aOR 1.15, 95% CI: 1.00 to 1.33) were associated with an increased POE risk.</p><p><strong>Conclusions: </strong>This study revealed that older age, higher American Society of Anesthesiology (ASA) stage, increasing severity of symptoms and ipsilateral moderate stenosis were associated with shorter prehospital delay. Non-specific symptoms were associated with a longer prehospital delay. Regarding in-hospital delay, older age, higher ASA stage, contralateral occlusion, preprocedural examination by a neurologist and admission on Fridays or Saturdays were associated with lagged treatment. A very short (<2 days) prehospital and intermediate in-hospital delay (2-3 days) were associated with increased risk of perioperative stroke or death.</p>","PeriodicalId":48733,"journal":{"name":"Journal of Investigative Medicine","volume":" ","pages":""},"PeriodicalIF":4.9000,"publicationDate":"2025-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12107447/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Investigative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2024-003098","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study analyses the determinants of prehospital (index event to admission) and in-hospital delay (admission to carotid endarterectomy (CEA)). In addition, the analysis addresses the association between prehospital or in-hospital delay and outcomes after CEA for symptomatic patients in German hospitals.
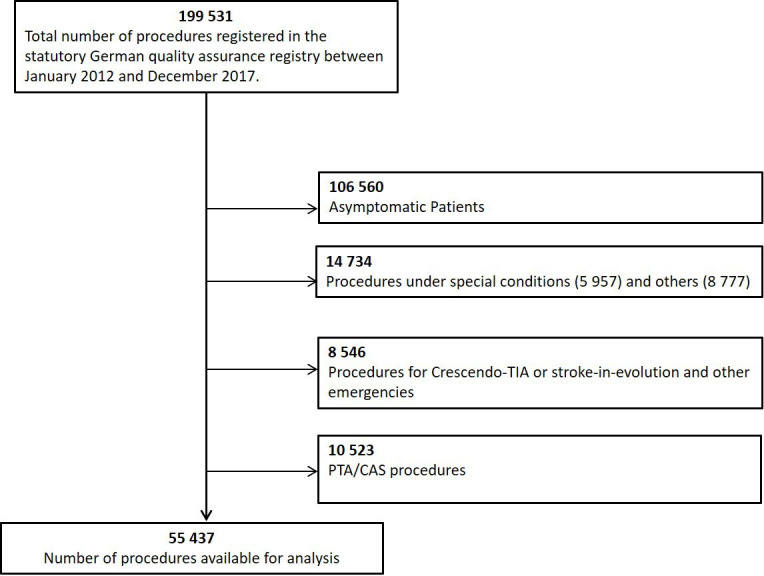
Materials and methods: This retrospective analysis is based on the nationwide German statutory quality assurance database. 55 437 patients were included in the analysis. Prehospital delay was grouped as follows: 180-15, 14-8, 7-3, 2-0 days or 'in-hospital index event'. In-hospital delay was divided into: 0-1, 2-3 and >3 days. The primary outcome event (POE) was in-hospital stroke or death. Univariate and multivariable regression analyses were performed for statistical analysis. The slope of the linear regression line is given as the β-value, and the rate parameter of the logistic regression is given as the adjusted OR (aOR).
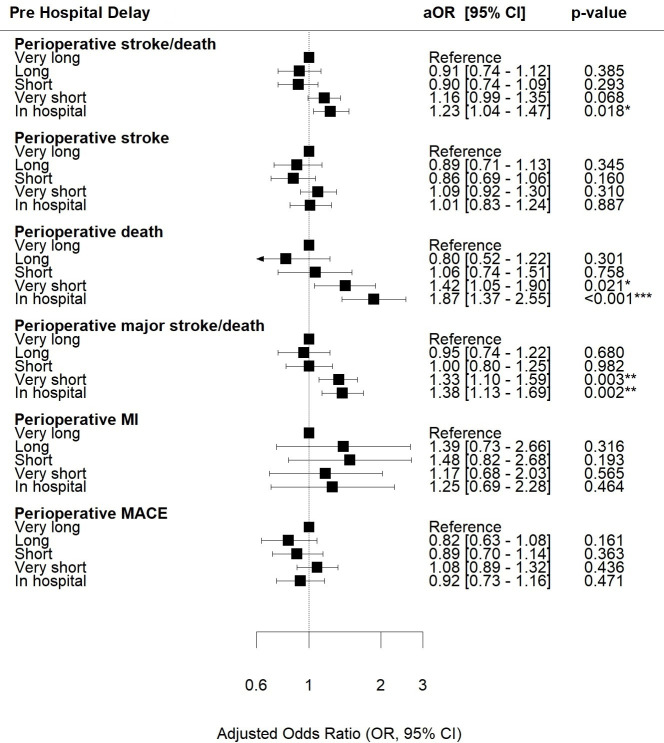
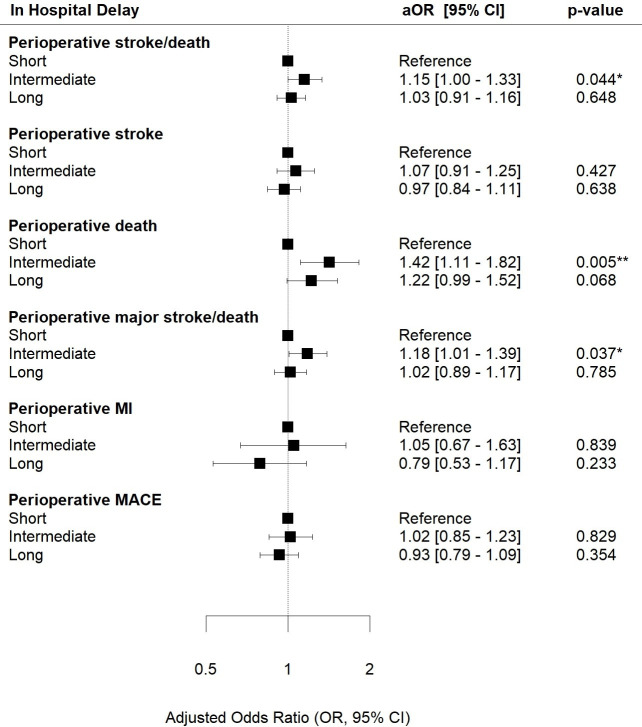
Results: Prehospital delay was 0-2 days in 34.9%, 3-14 days in 29.5% and >14 days in 18.6%. Higher age (β=-1.08, p<0.001) and a more severe index event (transitory ischaemic attack: β=-4.41, p<0.001; stroke: β=-6.05, p<0.001, Ref: amaurosis fugax) were determinants of shorter prehospital delay. Higher age (β=0.28, p<0.001) and female sex (β=0.09, p=0.014) were associated with a longer in-hospital delay. Index event after admission (aOR 1.23, 95% CI: 1.04 to 1.47) and an intermediate in-hospital delay of 2-3 days (aOR 1.15, 95% CI: 1.00 to 1.33) were associated with an increased POE risk.
Conclusions: This study revealed that older age, higher American Society of Anesthesiology (ASA) stage, increasing severity of symptoms and ipsilateral moderate stenosis were associated with shorter prehospital delay. Non-specific symptoms were associated with a longer prehospital delay. Regarding in-hospital delay, older age, higher ASA stage, contralateral occlusion, preprocedural examination by a neurologist and admission on Fridays or Saturdays were associated with lagged treatment. A very short (<2 days) prehospital and intermediate in-hospital delay (2-3 days) were associated with increased risk of perioperative stroke or death.
期刊介绍:
Journal of Investigative Medicine (JIM) is the official publication of the American Federation for Medical Research. The journal is peer-reviewed and publishes high-quality original articles and reviews in the areas of basic, clinical, and translational medical research.
JIM publishes on all topics and specialty areas that are critical to the conduct of the entire spectrum of biomedical research: from the translation of clinical observations at the bedside, to basic and animal research to clinical research and the implementation of innovative medical care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


