Adrián Alegre, Mercedes Gironella, Fernando Escalante, Juan M. Bergua, Carmen Martínez-Chamorro, Aurelio López, Esther González, Abelardo Bárez, Nieves Somolinos, Ernesto P. Persona, Alexia S. Cabrera, Alfons Soler, Belén I. Rodríguez, Joaquín M. López, Yolanda González, Verónica C. Giménez, Antonia Sampol, Carolina Muñoz, David Vilanova, Marta Durán, Carlos Fernández de Larrea, Spanish Myeloma Group (GEM_PETHEMA)
{"title":"Biological relapse in multiple myeloma: Outcome and treatment strategies in a Spanish real-world setting","authors":"Adrián Alegre, Mercedes Gironella, Fernando Escalante, Juan M. Bergua, Carmen Martínez-Chamorro, Aurelio López, Esther González, Abelardo Bárez, Nieves Somolinos, Ernesto P. Persona, Alexia S. Cabrera, Alfons Soler, Belén I. Rodríguez, Joaquín M. López, Yolanda González, Verónica C. Giménez, Antonia Sampol, Carolina Muñoz, David Vilanova, Marta Durán, Carlos Fernández de Larrea, Spanish Myeloma Group (GEM_PETHEMA)","doi":"10.1002/hem3.81","DOIUrl":null,"url":null,"abstract":"<p>Recommendations regarding the best time to start treatment in patients with relapsed/refractory multiple myeloma (RRMM) after biological relapse/progression (BR) are unclear. This observational, prospective, multicenter registry aimed to evaluate the impact on time to progression (TTP) of treatment initiation at BR versus at symptomatic clinical relapse (ClinR) based on the Spanish routine practice in adult patients with RRMM. Patients had two or less previous treatment lines and at least one previous partial response. Baseline characteristics and treatment outcomes were recorded, and survival was analyzed. Of 225 patients, 110 were treated at BR (TxBR group) and 115 at ClinR (TxClinR group) according to the investigators' criteria. The proportion of patients with higher ECOG, previous noncomplete remission (CR), and second relapse were significantly higher in the TxBR group compared to the TxClinR group. TheTxClinR group showed improved outcomes, including TTP, compared to the TxBR group. Progression-free survival increased in the TxClinR group (56.2 months) compared to the TxBR group (32.5 months) (<i>p</i> = 0.0137), and median overall survival also increased (<i>p</i> = 0.0897). Median TTP was significantly longer in patients relapsing from a CR (50.4 months) and in their first relapse (38.7 months) compared to those relapsing from a non-CR response (32.9 months) and in their second relapse (25.2 months). Physicians seemed to start treatment earlier in RRMM patients with poor prognosis features. Previous responses to anti-MM treatment and the number of prior treatment lines were identified as prognosis factors, whereby relapse from CR and first relapse were associated with a longer time to progression.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.81","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.81","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
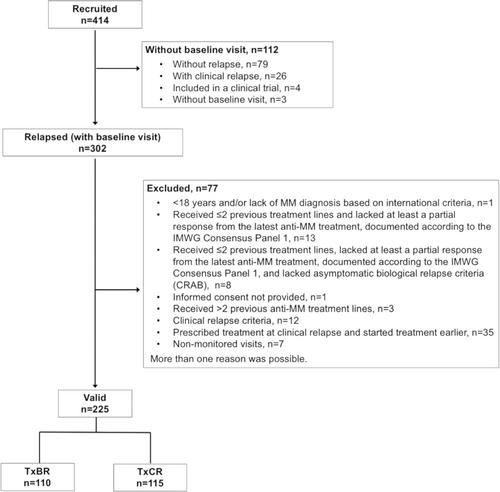
Recommendations regarding the best time to start treatment in patients with relapsed/refractory multiple myeloma (RRMM) after biological relapse/progression (BR) are unclear. This observational, prospective, multicenter registry aimed to evaluate the impact on time to progression (TTP) of treatment initiation at BR versus at symptomatic clinical relapse (ClinR) based on the Spanish routine practice in adult patients with RRMM. Patients had two or less previous treatment lines and at least one previous partial response. Baseline characteristics and treatment outcomes were recorded, and survival was analyzed. Of 225 patients, 110 were treated at BR (TxBR group) and 115 at ClinR (TxClinR group) according to the investigators' criteria. The proportion of patients with higher ECOG, previous noncomplete remission (CR), and second relapse were significantly higher in the TxBR group compared to the TxClinR group. TheTxClinR group showed improved outcomes, including TTP, compared to the TxBR group. Progression-free survival increased in the TxClinR group (56.2 months) compared to the TxBR group (32.5 months) (p = 0.0137), and median overall survival also increased (p = 0.0897). Median TTP was significantly longer in patients relapsing from a CR (50.4 months) and in their first relapse (38.7 months) compared to those relapsing from a non-CR response (32.9 months) and in their second relapse (25.2 months). Physicians seemed to start treatment earlier in RRMM patients with poor prognosis features. Previous responses to anti-MM treatment and the number of prior treatment lines were identified as prognosis factors, whereby relapse from CR and first relapse were associated with a longer time to progression.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


