{"title":"Medicare Eligibility and Changes in Coverage, Access to Care, and Health by Sexual Orientation and Gender Identity.","authors":"Kyle A Gavulic, Jacob Wallace","doi":"10.1001/jamahealthforum.2024.1756","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Medicare provides nearly universal insurance coverage at age 65 years. However, how Medicare eligibility affects disparities in health insurance coverage, access to care, and health status among individuals by sexual orientation and gender identity is poorly understood.</p><p><strong>Objective: </strong>To assess the association of Medicare eligibility with disparities in health insurance coverage, access to care, and self-reported health status among individuals by sexual orientation and by gender identity.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study used the age discontinuity for Medicare eligibility at age 65 years to isolate the association of Medicare with health insurance coverage, access to care, and self-reported health status, by their sexual orientation and by their gender identity. Data were collected from the Behavioral Risk Factor Surveillance System for respondents from 51 to 79 years old from 2014 to 2021. Data analysis was performed from September 2022 to April 2023.</p><p><strong>Exposures: </strong>Medicare eligibility at age 65 years.</p><p><strong>Main outcomes and measures: </strong>Proportions of respondents with health insurance coverage, usual source of care, cost barriers to care, influenza vaccination, and self-reported health status.</p><p><strong>Results: </strong>The study population included 927 952 individuals (mean [SD] age, 64.4 [7.7] years; 524 972 [56.6%] females and 402 670 [43.4%] males), of whom 28 077 (3.03%) identified as a sexual minority-lesbian, gay, bisexual, or another sexual minority identity (LGB+) and 3286 (0.35%) as transgender or gender diverse. Respondents who identified as heterosexual had greater improvements at age 65 years in insurance coverage (4.2 percentage points [pp]; 95% CI, 4.0-4.4 pp) than those who identified as LGB+ (3.6 pp; 95% CI, 2.3-4.8 pp), except when the analysis was limited to a subsample of married respondents. For access to care, improvements in usual source of care, cost barriers to care, and influenza vaccination were larger at age 65 years for heterosexual respondents compared with LGB+ respondents, although confidence intervals were overlapping and less precise for LGB+ individuals. For self-reported health status, the analyses found larger improvements at age 65 years for LGB+ respondents compared with heterosexual respondents. There was considerable heterogeneity by state in disparities by sexual orientation among individuals who were nearly eligible for Medicare (close to 65 years old), with the US South and Central states demonstrating the highest disparities. Among the top-10 highest-disparities states, Medicare eligibility was associated with greater increases in coverage (6.7 pp vs 5.0 pp) and access to a usual source of care (1.4 pp vs 0.6 pp) for LGB+ respondents compared with heterosexual respondents.</p><p><strong>Conclusions and relevance: </strong>The findings of this cross-sectional study indicate that Medicare eligibility was not associated with consistently greater improvements in health insurance coverage and access to care among LGBTQI+ individuals compared with heterosexual and/or cisgender individuals. However, among sexual minority individuals, Medicare may be associated with closing gaps in self-reported health status, and among states with the highest disparities, it may improve health insurance coverage, access to care, and self-reported health status.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"5 7","pages":"e241756"},"PeriodicalIF":11.3000,"publicationDate":"2024-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11227074/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2024.1756","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Medicare provides nearly universal insurance coverage at age 65 years. However, how Medicare eligibility affects disparities in health insurance coverage, access to care, and health status among individuals by sexual orientation and gender identity is poorly understood.
Objective: To assess the association of Medicare eligibility with disparities in health insurance coverage, access to care, and self-reported health status among individuals by sexual orientation and by gender identity.
Design, setting, and participants: This cross-sectional study used the age discontinuity for Medicare eligibility at age 65 years to isolate the association of Medicare with health insurance coverage, access to care, and self-reported health status, by their sexual orientation and by their gender identity. Data were collected from the Behavioral Risk Factor Surveillance System for respondents from 51 to 79 years old from 2014 to 2021. Data analysis was performed from September 2022 to April 2023.
Exposures: Medicare eligibility at age 65 years.
Main outcomes and measures: Proportions of respondents with health insurance coverage, usual source of care, cost barriers to care, influenza vaccination, and self-reported health status.
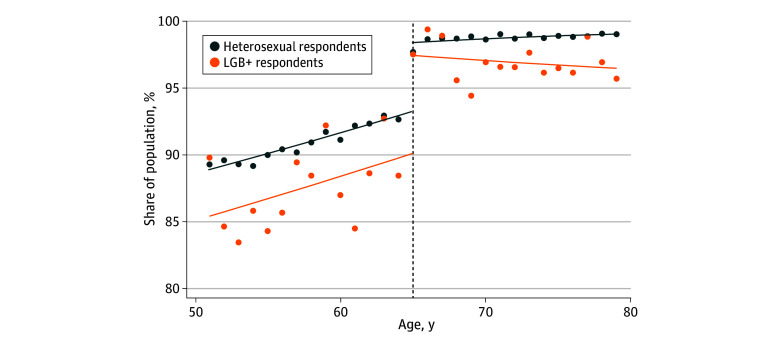
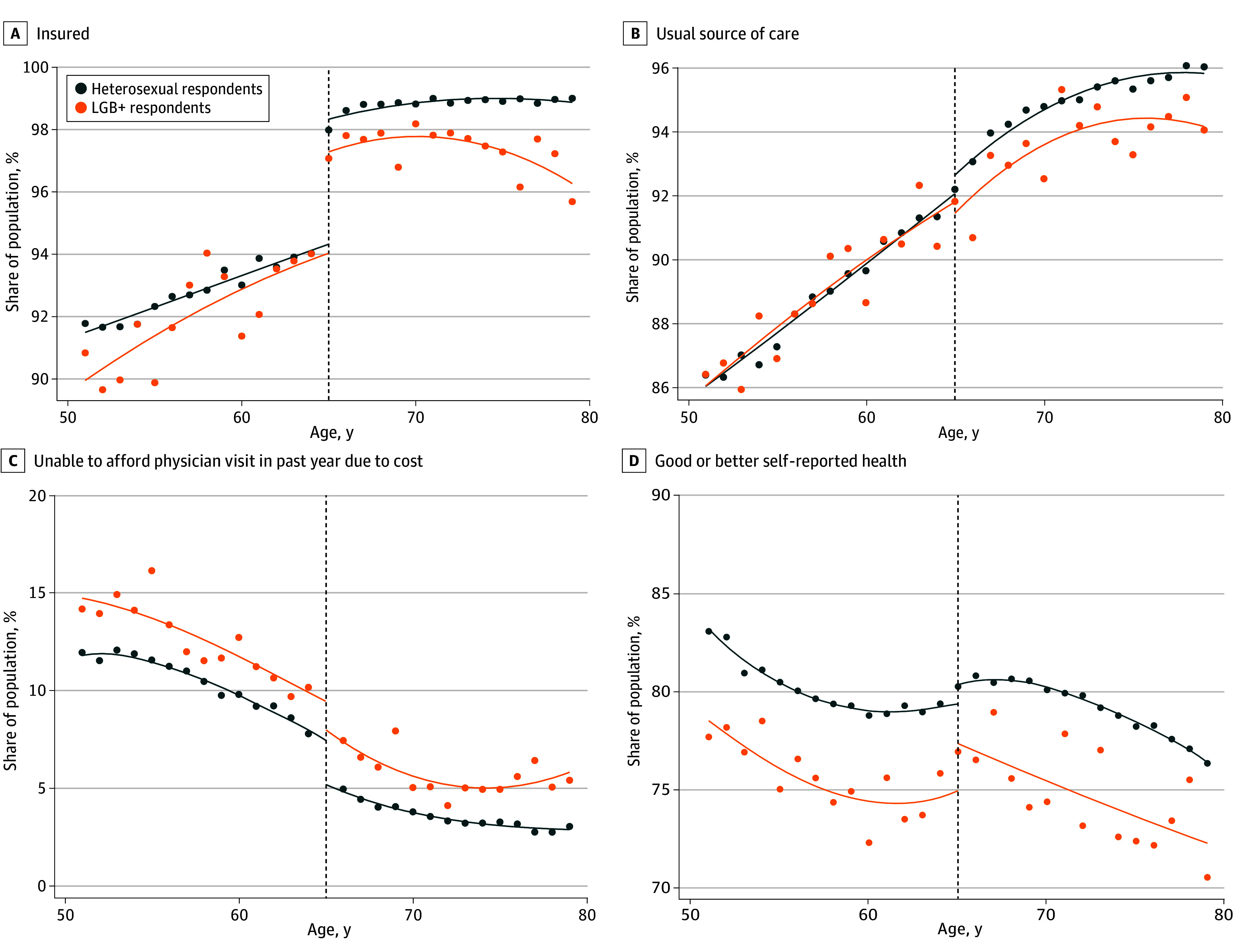
Results: The study population included 927 952 individuals (mean [SD] age, 64.4 [7.7] years; 524 972 [56.6%] females and 402 670 [43.4%] males), of whom 28 077 (3.03%) identified as a sexual minority-lesbian, gay, bisexual, or another sexual minority identity (LGB+) and 3286 (0.35%) as transgender or gender diverse. Respondents who identified as heterosexual had greater improvements at age 65 years in insurance coverage (4.2 percentage points [pp]; 95% CI, 4.0-4.4 pp) than those who identified as LGB+ (3.6 pp; 95% CI, 2.3-4.8 pp), except when the analysis was limited to a subsample of married respondents. For access to care, improvements in usual source of care, cost barriers to care, and influenza vaccination were larger at age 65 years for heterosexual respondents compared with LGB+ respondents, although confidence intervals were overlapping and less precise for LGB+ individuals. For self-reported health status, the analyses found larger improvements at age 65 years for LGB+ respondents compared with heterosexual respondents. There was considerable heterogeneity by state in disparities by sexual orientation among individuals who were nearly eligible for Medicare (close to 65 years old), with the US South and Central states demonstrating the highest disparities. Among the top-10 highest-disparities states, Medicare eligibility was associated with greater increases in coverage (6.7 pp vs 5.0 pp) and access to a usual source of care (1.4 pp vs 0.6 pp) for LGB+ respondents compared with heterosexual respondents.
Conclusions and relevance: The findings of this cross-sectional study indicate that Medicare eligibility was not associated with consistently greater improvements in health insurance coverage and access to care among LGBTQI+ individuals compared with heterosexual and/or cisgender individuals. However, among sexual minority individuals, Medicare may be associated with closing gaps in self-reported health status, and among states with the highest disparities, it may improve health insurance coverage, access to care, and self-reported health status.
医疗保险资格以及按性取向和性别认同划分的承保范围、获得护理的机会和健康状况的变化》(Medicare Eligibility and Changes in Coverage, Access to Care, and Health by Sexual Orientation and Gender Identity)。
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


