Using FRAME to characterize provider-identified adaptations to a stepped care intervention for adolescents and youth living with HIV in Kenya: a mixed methods approach
Abstract
Introduction
The Data-informed Stepped Care (DiSC) study is a cluster-randomized trial implemented in 24 HIV care clinics in Kenya, aimed at improving retention in care for adolescents and youth living with HIV (AYLHIV). DiSC is a multi-component intervention that assigns AYLHIV to different intensity (steps) of services according to risk. We used the Framework for Reporting Adaptations and Modifications-Expanded (FRAME) to characterize provider-identified adaptations to the implementation of DiSC to optimize uptake and delivery, and determine the influence on implementation outcomes.
Methods
Between May and December 2022, we conducted continuous quality improvement (CQI) meetings with providers to optimize DiSC implementation at 12 intervention sites. The meetings were guided by plan-do-study-act processes to identify challenges during early phase implementation and propose targeted adaptations. Meetings were audio-recorded and analysed using FRAME to categorize the level, context and content of planned adaptations and determine if adaptations were fidelity consistent. Providers completed surveys to quantify perceptions of DiSC acceptability, appropriateness and feasibility. Mixed effects linear regression models were used to evaluate these implementation outcomes over time.
Results
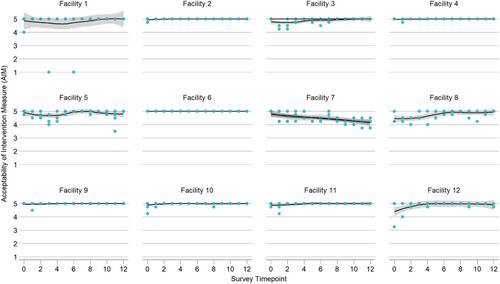
Providers participated in eight CQI meetings per facility over a 6-month period. A total of 65 adaptations were included in the analysis. The majority focused on optimizing the integration of DiSC within the clinic (83%, n = 54), and consisted of improving documentation, addressing scheduling challenges and improving clinic workflow. Primary reasons for adaptation were to align delivery with AYLHIV needs and preferences and to increase reach among AYLHIV: with reminder calls to AYLHIV, collaborating with schools to ensure AYLHIV attended clinic appointments and addressing transportation challenges. All adaptations to optimize DiSC implementation were fidelity-consistent. Provider perceptions of implementation were consistently high throughout the process, and on average, slightly improved each month for intervention acceptability (β = 0.011, 95% CI: 0.002, 0.020, p = 0.016), appropriateness (β = 0.012, 95% CI: 0.007, 0.027, p<0.001) and feasibility (β = 0.013, 95% CI: 0.004, 0.022, p = 0.005).
Conclusions
Provider-identified adaptations targeted improved integration into routine clinic practices and aimed to reduce barriers to service access unique to AYLHIV. Characterizing types of adaptations and adaptation rationale may enrich our understanding of the implementation context and improve abilities to tailor implementation strategies when scaling to new settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


