Lianqin Zhang, Kang Zhou, Tianchu Gu, Jingjing Xu, Mengzhu Shi, Jiang Zhu, Jindong Liu
{"title":"Cardiopulmonary Protection of Modified Remote Ischemic Preconditioning in Mitral Valve Replacement Surgery: A Randomized Controlled Trial","authors":"Lianqin Zhang, Kang Zhou, Tianchu Gu, Jingjing Xu, Mengzhu Shi, Jiang Zhu, Jindong Liu","doi":"10.1155/2024/9889995","DOIUrl":null,"url":null,"abstract":"<p><b>Background:</b> Remote ischemic preconditioning (RIPC) is reported to have early-phase and delayed-phase organ-protective effects. Previous studies have focused on the organ protection of a single RIPC protocol, and the clinical outcomes remain uncertain. Whether the modified RIPC (mRIPC) protocol performed repeatedly provides cardiopulmonary protection is still uncertain.</p><p><b>Methods:</b> In this single-center, randomized, controlled trial, 86 patients undergoing elective mitral valve replacement (MVR) surgery were randomized 1:1 to receive either mRIPC or no ischemic preconditioning (control). Three cycles of 5 min ischemia and 5 min reperfusion induced by a blood pressure cuff served as the RIPC stimulus. mRIPC was induced at the following three time points: 24 h, 12 h, and 1 h before surgery. Blood samples were withdrawn at 10 min after intubation (T0), at 1 h after aortic declamping (T1), and at 6 h (T2), 12 h (T3), and 24 h (T4) after surgery to measure the serum concentrations of myocardial enzymes and other biomarkers, including cardiac troponin I (cTnI), which was the primary endpoint of this study. Creatine kinase isoenzyme (CK-MB), lactate dehydrogenase (LDH), inotropic score (IS), and inflammatory mediators were also measured. Blood gas analysis was conducted to calculate the PaO<sub>2</sub>/FiO<sub>2</sub> ratio and A-aDO<sub>2</sub>, and the incidence of acute lung injury (ALI) was also recorded.</p><p><b>Results:</b> mRIPC significantly decreased the serum concentrations of cTnI, CK-MB, and LDH at T2, T3, and T4 (<i>p</i> < 0.01), and the IS decreased compared with that in the control group (12.0 ± 1.0 vs. 14.2 ± 1.1, <i>p</i> < 0.01). In addition, the incidence of ALI in the mRIPC group was decreased (32.6% vs. 51.2%, <i>p</i> = 0.039), and the PaO<sub>2</sub>/FiO<sub>2</sub> was higher at T4 (<i>p</i> < 0.05). Compared with those in the control group, the levels of interleukin-6 (IL-6) and tumor necrosis factor-<i>α</i> (TNF-<i>α</i>) were decreased at T1, T2, T3, and T4 (<i>p</i> < 0.05) in the mRIPC group, and the level of IL-10 increased at the same time.</p><p><b>Conclusions:</b> mRIPC decreased the incidence of myocardial and lung injury in MVR surgery, providing new evidence for the clinical application of RIPC in valve surgery.</p><p><b>Trial Registration:</b> ClinicalTrials.gov (NCT01406678).</p>","PeriodicalId":9582,"journal":{"name":"Cardiovascular Therapeutics","volume":"2024 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/9889995","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/9889995","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Remote ischemic preconditioning (RIPC) is reported to have early-phase and delayed-phase organ-protective effects. Previous studies have focused on the organ protection of a single RIPC protocol, and the clinical outcomes remain uncertain. Whether the modified RIPC (mRIPC) protocol performed repeatedly provides cardiopulmonary protection is still uncertain.
Methods: In this single-center, randomized, controlled trial, 86 patients undergoing elective mitral valve replacement (MVR) surgery were randomized 1:1 to receive either mRIPC or no ischemic preconditioning (control). Three cycles of 5 min ischemia and 5 min reperfusion induced by a blood pressure cuff served as the RIPC stimulus. mRIPC was induced at the following three time points: 24 h, 12 h, and 1 h before surgery. Blood samples were withdrawn at 10 min after intubation (T0), at 1 h after aortic declamping (T1), and at 6 h (T2), 12 h (T3), and 24 h (T4) after surgery to measure the serum concentrations of myocardial enzymes and other biomarkers, including cardiac troponin I (cTnI), which was the primary endpoint of this study. Creatine kinase isoenzyme (CK-MB), lactate dehydrogenase (LDH), inotropic score (IS), and inflammatory mediators were also measured. Blood gas analysis was conducted to calculate the PaO2/FiO2 ratio and A-aDO2, and the incidence of acute lung injury (ALI) was also recorded.
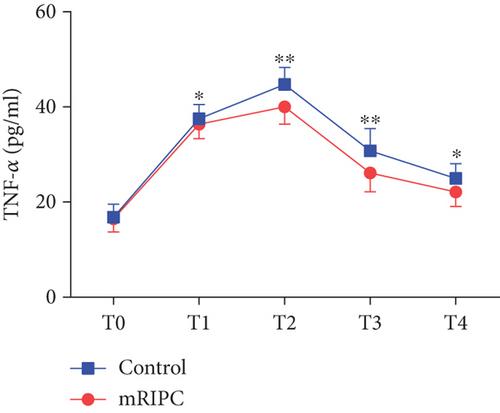
Results: mRIPC significantly decreased the serum concentrations of cTnI, CK-MB, and LDH at T2, T3, and T4 (p < 0.01), and the IS decreased compared with that in the control group (12.0 ± 1.0 vs. 14.2 ± 1.1, p < 0.01). In addition, the incidence of ALI in the mRIPC group was decreased (32.6% vs. 51.2%, p = 0.039), and the PaO2/FiO2 was higher at T4 (p < 0.05). Compared with those in the control group, the levels of interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) were decreased at T1, T2, T3, and T4 (p < 0.05) in the mRIPC group, and the level of IL-10 increased at the same time.
Conclusions: mRIPC decreased the incidence of myocardial and lung injury in MVR surgery, providing new evidence for the clinical application of RIPC in valve surgery.
期刊介绍:
Cardiovascular Therapeutics (formerly Cardiovascular Drug Reviews) is a peer-reviewed, Open Access journal that publishes original research and review articles focusing on cardiovascular and clinical pharmacology, as well as clinical trials of new cardiovascular therapies. Articles on translational research, pharmacogenomics and personalized medicine, device, gene and cell therapies, and pharmacoepidemiology are also encouraged.
Subject areas include (but are by no means limited to):
Acute coronary syndrome
Arrhythmias
Atherosclerosis
Basic cardiac electrophysiology
Cardiac catheterization
Cardiac remodeling
Coagulation and thrombosis
Diabetic cardiovascular disease
Heart failure (systolic HF, HFrEF, diastolic HF, HFpEF)
Hyperlipidemia
Hypertension
Ischemic heart disease
Vascular biology
Ventricular assist devices
Molecular cardio-biology
Myocardial regeneration
Lipoprotein metabolism
Radial artery access
Percutaneous coronary intervention
Transcatheter aortic and mitral valve replacement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


