Erin R McKnight, Ashley Ebersole, James Gallup, Fareeda W Haamid
{"title":"Developing a Sustainable Quality Improvement Program in an Academic Center: The Experience of an Adolescent Unit.","authors":"Erin R McKnight, Ashley Ebersole, James Gallup, Fareeda W Haamid","doi":"10.1097/pq9.0000000000000742","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Successful quality improvement (QI) efforts use a comprehensive, institutional QI framework and professional development, but literature describing implementing QI frameworks in Adolescent Medicine practices is sparse. We aimed to implement and increase the number of formally structured QI projects (primary aim) and the number of projects achieving a centerline (CL) shift (secondary aim) in our hospital's Adolescent Medicine Clinic.</p><p><strong>Methods: </strong>We used formal QI methodology to improve health outcomes by increasing the number of faculty with formalized QI education, creating interdisciplinary QI teams, and improving staff motivation. QI education was mandatory for Adolescent Medicine fellows and pediatric residents and encouraged for faculty and staff. The Divisional QI leadership team attended monthly meetings to review key driver diagrams, run and control charts, and receive intervention updates. All providers and staff received monthly updates, and the Hospital Quality and Safety Committee received biannual updates. We used run charts to share progress with primary and secondary aims.</p><p><strong>Results: </strong>Since Q3 2014, the Adolescent Medicine team consistently achieved the primary aim of having 5 active projects in process, with 9 projects from Q1 2018-Q4 2020. For the secondary aim, a target of 50% of active QI projects attaining a sustained centerline shift was achieved in Q2 2018 and maintained in 16 of 20 quarters since.</p><p><strong>Conclusions: </strong>Clinicians can use QI methodology to improve health outcomes while facilitating professional development. For this initiative to succeed, institutional leadership must provide an infrastructure prioritizing meaningful QI involvement.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e742"},"PeriodicalIF":1.1000,"publicationDate":"2024-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11167228/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000742","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
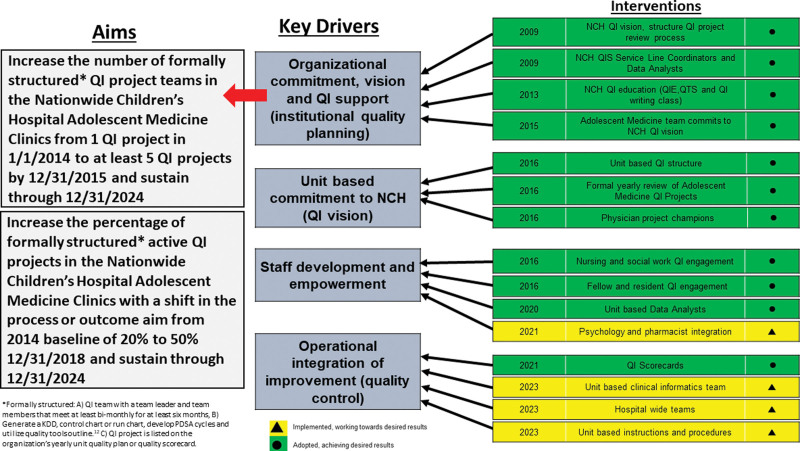
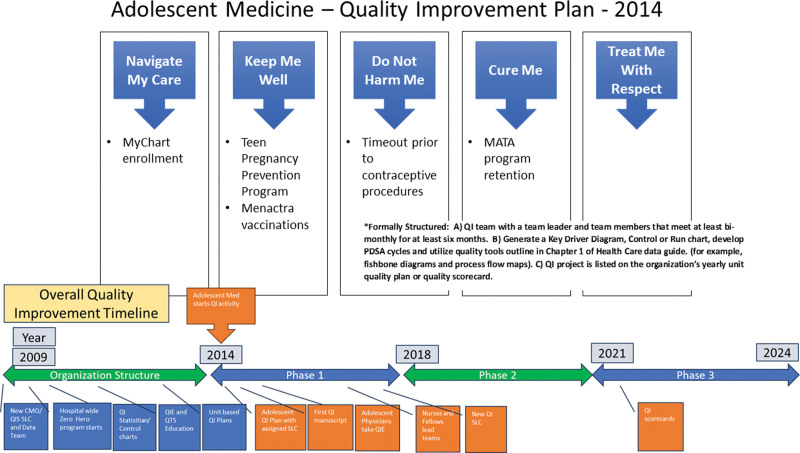
Introduction: Successful quality improvement (QI) efforts use a comprehensive, institutional QI framework and professional development, but literature describing implementing QI frameworks in Adolescent Medicine practices is sparse. We aimed to implement and increase the number of formally structured QI projects (primary aim) and the number of projects achieving a centerline (CL) shift (secondary aim) in our hospital's Adolescent Medicine Clinic.
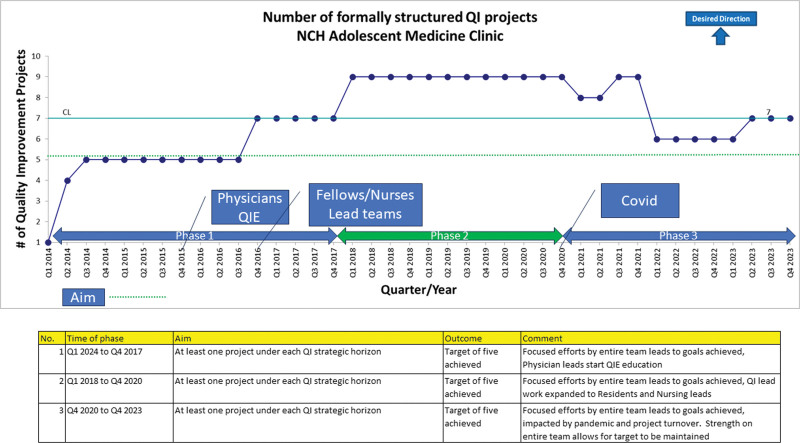
Methods: We used formal QI methodology to improve health outcomes by increasing the number of faculty with formalized QI education, creating interdisciplinary QI teams, and improving staff motivation. QI education was mandatory for Adolescent Medicine fellows and pediatric residents and encouraged for faculty and staff. The Divisional QI leadership team attended monthly meetings to review key driver diagrams, run and control charts, and receive intervention updates. All providers and staff received monthly updates, and the Hospital Quality and Safety Committee received biannual updates. We used run charts to share progress with primary and secondary aims.
Results: Since Q3 2014, the Adolescent Medicine team consistently achieved the primary aim of having 5 active projects in process, with 9 projects from Q1 2018-Q4 2020. For the secondary aim, a target of 50% of active QI projects attaining a sustained centerline shift was achieved in Q2 2018 and maintained in 16 of 20 quarters since.
Conclusions: Clinicians can use QI methodology to improve health outcomes while facilitating professional development. For this initiative to succeed, institutional leadership must provide an infrastructure prioritizing meaningful QI involvement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


