Harry Mee, J M Harris, T Korhonen, F Anwar, A J Wahba, Michael Martin, G Whiting, E Viaroli, I Timofeev, A Helmy, Angelos G Kolias, Peter J Hutchinson
{"title":"Decompressive craniectomy to cranioplasty: a retrospective observational study using Hospital Episode Statistics in England.","authors":"Harry Mee, J M Harris, T Korhonen, F Anwar, A J Wahba, Michael Martin, G Whiting, E Viaroli, I Timofeev, A Helmy, Angelos G Kolias, Peter J Hutchinson","doi":"10.1136/bmjsit-2023-000253","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the longitudinal trends of decompressive craniectomy (DC) following traumatic brain injury (TBI) or stroke and explore whether the timing of cranial reconstruction affected revision or removal rates using Hospital Episode Statistics (HES) between 2014 and 2019.</p><p><strong>Design: </strong>Retrospective observational cohort study using HES. The time frame definitions mirror those often used in clinical practice.</p><p><strong>Setting: </strong>HES data from neurosurgical centres in England.</p><p><strong>Participants: </strong>HES data related to decompressive craniectomy procedures and cranioplasty following TBI or stroke between 2014 and 2019.</p><p><strong>Main outcome measures: </strong>The primary outcome was the timing and rate of revision/removal compared with cranioplasty within <12 weeks to ≥12 weeks.</p><p><strong>Results: </strong>There were 4627 DC procedures, of which 1847 (40%) were due to head injury, 1116 (24%) were due to stroke, 728 (16%) were due to other cerebrovascular diagnoses, 317 (7%) had mixed diagnosis and 619 (13%) had no pre-specified diagnoses. The number of DC procedures performed per year ranged from 876 in 2014-2015 to 967 in 2018-2019. There were 4466 cranioplasty procedures, with 309 (7%) revisions and/or removals during the first postoperative year. There was a 33% increase in the overall number of cranioplasty procedures performed within 12 weeks, and there were 1823 patients who underwent both craniectomy and cranioplasty during the study period, with 1436 (79%) having a cranioplasty within 1 year. However, relating to the timing of cranial reconstruction, there was no evidence of any difference in the rate of revision or removal surgery in the early timing group (6.5%) compared with standard care (7.9%) (adjusted HR 0.93, 95% CIs 0.61 to 1.43; p=0.75).</p><p><strong>Conclusions: </strong>Overall number of craniectomies and the subsequent requirements for cranioplasty increased steadily during the study period. However, relating to the timing of cranial reconstruction, there was no evidence of an overall difference in the rate of revision or removal surgery in the early timing group.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"6 1","pages":"e000253"},"PeriodicalIF":1.6000,"publicationDate":"2024-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11149159/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2023-000253","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To investigate the longitudinal trends of decompressive craniectomy (DC) following traumatic brain injury (TBI) or stroke and explore whether the timing of cranial reconstruction affected revision or removal rates using Hospital Episode Statistics (HES) between 2014 and 2019.
Design: Retrospective observational cohort study using HES. The time frame definitions mirror those often used in clinical practice.
Setting: HES data from neurosurgical centres in England.
Participants: HES data related to decompressive craniectomy procedures and cranioplasty following TBI or stroke between 2014 and 2019.
Main outcome measures: The primary outcome was the timing and rate of revision/removal compared with cranioplasty within <12 weeks to ≥12 weeks.
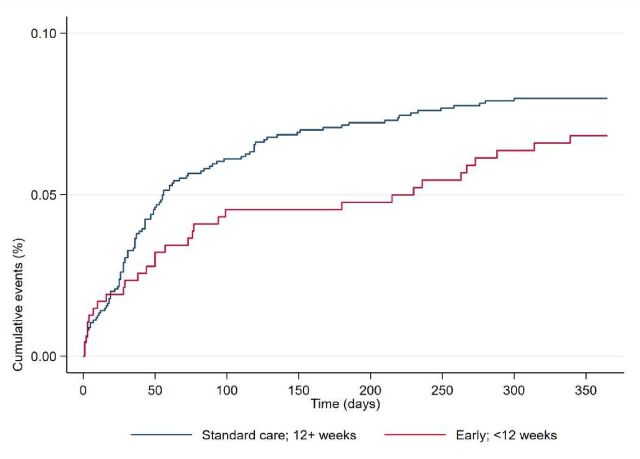
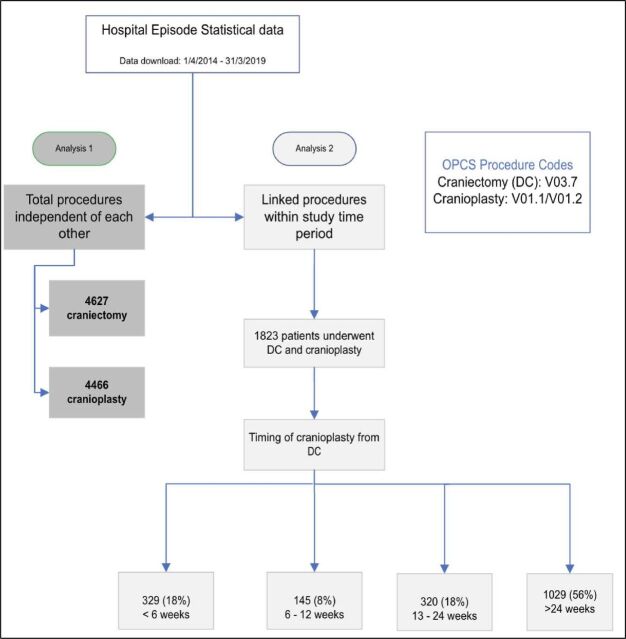
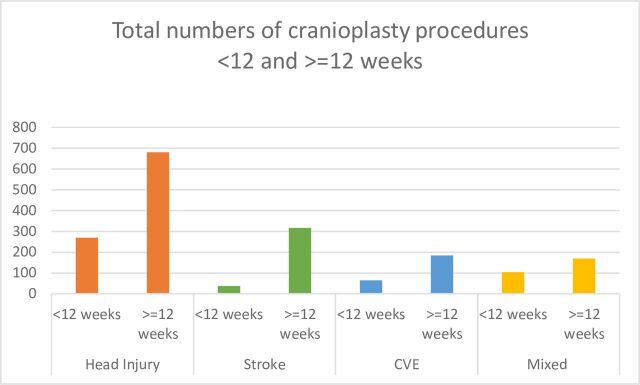
Results: There were 4627 DC procedures, of which 1847 (40%) were due to head injury, 1116 (24%) were due to stroke, 728 (16%) were due to other cerebrovascular diagnoses, 317 (7%) had mixed diagnosis and 619 (13%) had no pre-specified diagnoses. The number of DC procedures performed per year ranged from 876 in 2014-2015 to 967 in 2018-2019. There were 4466 cranioplasty procedures, with 309 (7%) revisions and/or removals during the first postoperative year. There was a 33% increase in the overall number of cranioplasty procedures performed within 12 weeks, and there were 1823 patients who underwent both craniectomy and cranioplasty during the study period, with 1436 (79%) having a cranioplasty within 1 year. However, relating to the timing of cranial reconstruction, there was no evidence of any difference in the rate of revision or removal surgery in the early timing group (6.5%) compared with standard care (7.9%) (adjusted HR 0.93, 95% CIs 0.61 to 1.43; p=0.75).
Conclusions: Overall number of craniectomies and the subsequent requirements for cranioplasty increased steadily during the study period. However, relating to the timing of cranial reconstruction, there was no evidence of an overall difference in the rate of revision or removal surgery in the early timing group.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


