Pududu Archie Rachuene, Roopam Dey, Ntambue Jimmy Kauta, Sudesh Sivarasu, Jean-Pierre du Plessis, Stephen Roche, Basil Vrettos
{"title":"Pre-operative planning for reverse shoulder arthroplasty in low-resource centres: A modified Delphi study in South Africa.","authors":"Pududu Archie Rachuene, Roopam Dey, Ntambue Jimmy Kauta, Sudesh Sivarasu, Jean-Pierre du Plessis, Stephen Roche, Basil Vrettos","doi":"10.1051/sicotj/2024021","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pre-operative planning for reverse shoulder arthroplasty (RSA) poses challenges, particularly when dealing with glenoid bone loss. This modified Delphi study aimed to assess expert consensus on RSA planning processes and rationale, specifically targeting low-resourced institutions. Our objective was to offer pre-operative decision-making algorithms tailored for surgeons practising in resource-constrained hospitals with limited access to computed tomography (CT) scans.</p><p><strong>Methods: </strong>A working group generated statements on pre-operative imaging and glenoid of glenoid morphology and intra-operative decision-making. The study was conducted in three stages, with virtual consensus meetings in between. Stages 2 and 3 consisted only of closed questions/statements. The statements with over 70% were considered consensus achieved and those with less than 10% were considered disagreement consensus achieved.</p><p><strong>Results: </strong>Twelve shoulder surgeons participated, with 67% having over five years of experience in shoulder arthroplasty. In the absence of glenoid bone loss, the sole use of plain radiographs for pre-operative planning reached consensus and is recommended by these groups, while 100% advise using CT scans when bone loss is present. Most surgeons (70%) recommend using patient-specific instrumentation (PSI) in cases of structural bone loss. Most of the statements on intra-operative decision-making related to component placement and enhancing stability failed to reach consensus.</p><p><strong>Conclusion: </strong>While consensus was achieved on most aspects of pre-operative imaging and planning, technical aspects of surgery lacked consensus. Planning for patients with structural glenoid bone loss necessitates CT scans and planning tools.</p>","PeriodicalId":46378,"journal":{"name":"SICOT-J","volume":"10 ","pages":"23"},"PeriodicalIF":2.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11141516/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SICOT-J","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/sicotj/2024021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pre-operative planning for reverse shoulder arthroplasty (RSA) poses challenges, particularly when dealing with glenoid bone loss. This modified Delphi study aimed to assess expert consensus on RSA planning processes and rationale, specifically targeting low-resourced institutions. Our objective was to offer pre-operative decision-making algorithms tailored for surgeons practising in resource-constrained hospitals with limited access to computed tomography (CT) scans.
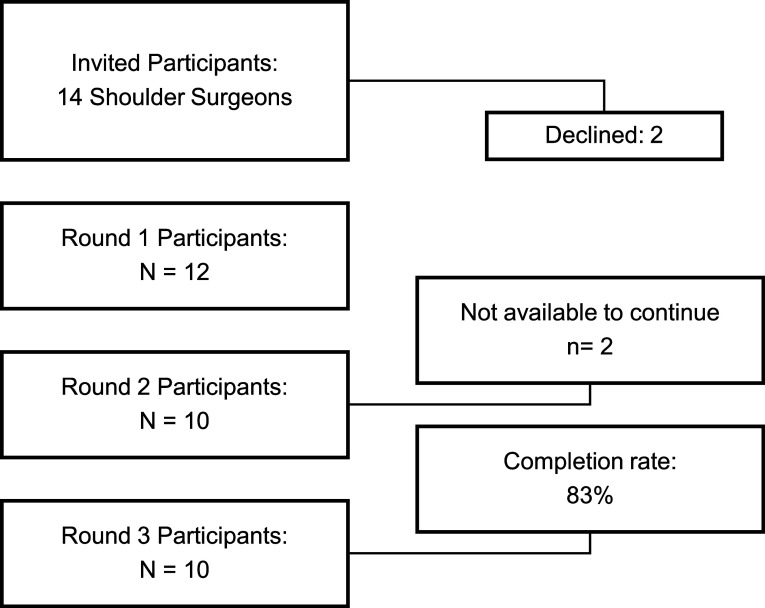
Methods: A working group generated statements on pre-operative imaging and glenoid of glenoid morphology and intra-operative decision-making. The study was conducted in three stages, with virtual consensus meetings in between. Stages 2 and 3 consisted only of closed questions/statements. The statements with over 70% were considered consensus achieved and those with less than 10% were considered disagreement consensus achieved.
Results: Twelve shoulder surgeons participated, with 67% having over five years of experience in shoulder arthroplasty. In the absence of glenoid bone loss, the sole use of plain radiographs for pre-operative planning reached consensus and is recommended by these groups, while 100% advise using CT scans when bone loss is present. Most surgeons (70%) recommend using patient-specific instrumentation (PSI) in cases of structural bone loss. Most of the statements on intra-operative decision-making related to component placement and enhancing stability failed to reach consensus.
Conclusion: While consensus was achieved on most aspects of pre-operative imaging and planning, technical aspects of surgery lacked consensus. Planning for patients with structural glenoid bone loss necessitates CT scans and planning tools.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


