Chris Bojke, David Cottrell, Alex Wright-Hughes, Amanda Farrin, Sandy Tubeuf
{"title":"Long-term cost-utility analysis of family therapy vs. treatment as usual for young people seen after self-harm.","authors":"Chris Bojke, David Cottrell, Alex Wright-Hughes, Amanda Farrin, Sandy Tubeuf","doi":"10.1186/s12962-024-00546-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The joint evidence of the cost and the effectiveness of family-based therapies is modest.</p><p><strong>Objective: </strong>To study the cost-effectiveness of family therapy (FT) versus treatment-as-usual (TAU) for young people seen after self-harm combining data from an 18-month trial and hospital records up to 60-month from randomisation.</p><p><strong>Methods: </strong>We estimate the cost-effectiveness of FT compared to TAU over 5 years using a quasi-Markov state model based on self-harm hospitalisations where probabilities of belonging in a state are directly estimated from hospital data. The primary outcome is quality-adjusted life years (QALY). Cost perspective is NHS and PSS and includes treatment costs, health care use, and hospital attendances whether it is for self-harm or not. Incremental cost-effectiveness ratios are calculated and deterministic and probabilistic sensitivity analyses are conducted.</p><p><strong>Results: </strong>Both trial arms show a significant decrease in hospitalisations over the 60-month follow-up. In the base case scenario, FT participants incur higher costs (mean +£1,693) and negative incremental QALYs (-0.01) than TAU patients. The associated ICER at 5 years is dominated and the incremental health benefit at the £30,000 per QALY threshold is -0.067. Probabilistic Sensitivity Analysis finds the probability that FT is cost-effective is around 3 - 2% up to a maximum willingness to pay of £50,000 per QALY. This suggest that the extension of the data to 60 months show no difference in effectiveness between treatments.</p><p><strong>Conclusion: </strong>Whilst extended trial follow-up from routinely collected statistics is useful to improve the modelling of longer-term cost-effectiveness, FT is not cost-effective relative to TAU and dominated in a cost-utility analysis.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"22 1","pages":"49"},"PeriodicalIF":2.5000,"publicationDate":"2024-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11138073/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-024-00546-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The joint evidence of the cost and the effectiveness of family-based therapies is modest.
Objective: To study the cost-effectiveness of family therapy (FT) versus treatment-as-usual (TAU) for young people seen after self-harm combining data from an 18-month trial and hospital records up to 60-month from randomisation.
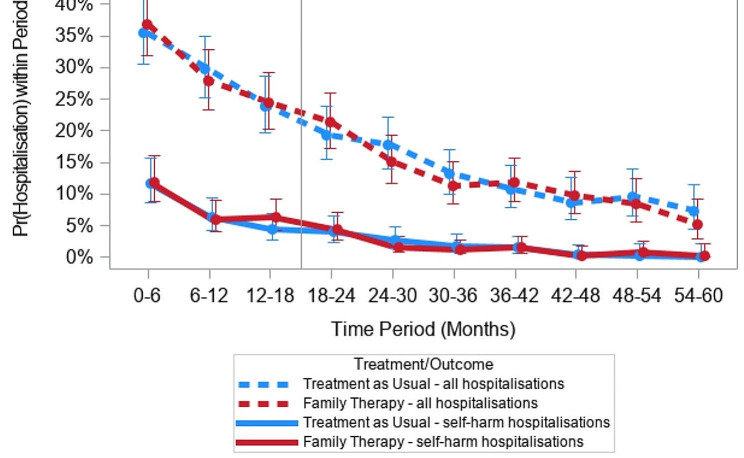
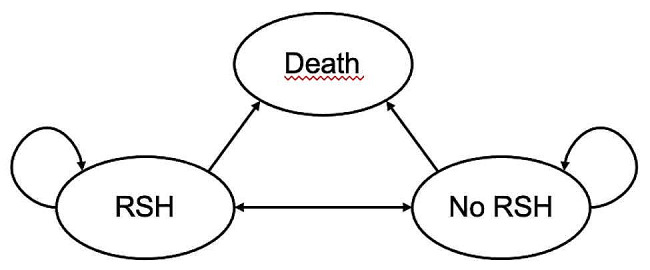
Methods: We estimate the cost-effectiveness of FT compared to TAU over 5 years using a quasi-Markov state model based on self-harm hospitalisations where probabilities of belonging in a state are directly estimated from hospital data. The primary outcome is quality-adjusted life years (QALY). Cost perspective is NHS and PSS and includes treatment costs, health care use, and hospital attendances whether it is for self-harm or not. Incremental cost-effectiveness ratios are calculated and deterministic and probabilistic sensitivity analyses are conducted.
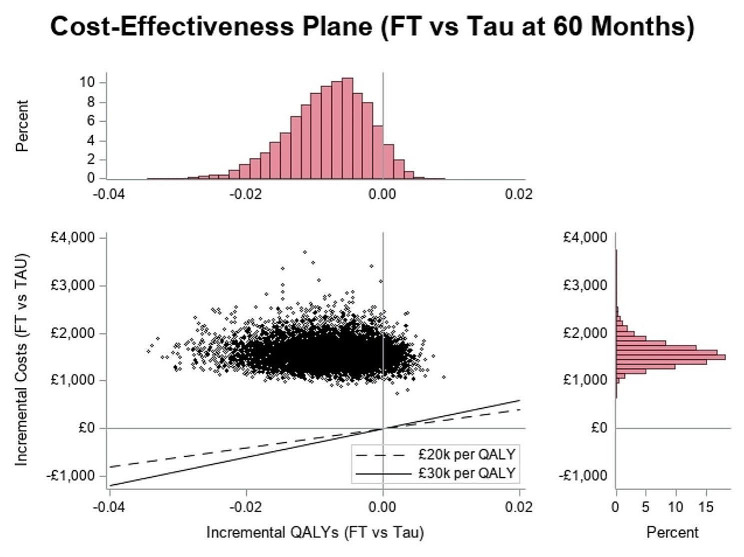
Results: Both trial arms show a significant decrease in hospitalisations over the 60-month follow-up. In the base case scenario, FT participants incur higher costs (mean +£1,693) and negative incremental QALYs (-0.01) than TAU patients. The associated ICER at 5 years is dominated and the incremental health benefit at the £30,000 per QALY threshold is -0.067. Probabilistic Sensitivity Analysis finds the probability that FT is cost-effective is around 3 - 2% up to a maximum willingness to pay of £50,000 per QALY. This suggest that the extension of the data to 60 months show no difference in effectiveness between treatments.
Conclusion: Whilst extended trial follow-up from routinely collected statistics is useful to improve the modelling of longer-term cost-effectiveness, FT is not cost-effective relative to TAU and dominated in a cost-utility analysis.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


