Elizabeth A Mann, Kelsi Alexander, Whitney Beaton, Elizabeth B Roe, Amy Grant, Kristin A Shadman
{"title":"Screening for Nephropathy in Pediatric Type 2 Diabetes: Quality Improvement to Increase Nephropathy Screening.","authors":"Elizabeth A Mann, Kelsi Alexander, Whitney Beaton, Elizabeth B Roe, Amy Grant, Kristin A Shadman","doi":"10.1097/pq9.0000000000000734","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Screening for early detection of microalbuminuria signaling kidney disease should begin as early as the time of diagnosis of youth-onset type 2 diabetes. This quality improvement initiative aimed to standardize urine nephropathy screening in pediatric patients with type 2 diabetes at a tertiary academic medical center and increase a baseline screening rate of 56%-75% over 6 months (September 2022-February 2023) and sustain that increase for 6 months (March through August 2023).</p><p><strong>Methods: </strong>A multi-disciplinary team used quality improvement methods and iterative Plan-Do-Study-Act cycles. Targeted interventions included previsit planning workflow, education, and a new-onset triage protocol. The team collected data at baseline and prospectively by reviewing electronic medical records. The primary outcome measure was pediatric type 2 diabetes clinic visits in diabetes clinic with urine nephropathy screening before or on the visit date.</p><p><strong>Results: </strong>A total of 121 youth were scheduled for T2D clinic visits between September 2021 and August 2023. The mean age was 14.5 years, and 60% were women, 40% were non-Hispanic Black, 28% were Hispanic/Latino, and 15% reported Spanish as their preferred language. Following the interventions of this project, urine nephropathy screening increased from 56% to 75%, and this change was sustained for 6 months.</p><p><strong>Conclusions: </strong>Interventions focused on efficient recognition of the population needing screening, coordinated internal processes around screening, a shared understanding between all stakeholders, and practical support in the healthcare system increased urine nephropathy screening with sustained improvement.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e734"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11132389/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000734","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Screening for early detection of microalbuminuria signaling kidney disease should begin as early as the time of diagnosis of youth-onset type 2 diabetes. This quality improvement initiative aimed to standardize urine nephropathy screening in pediatric patients with type 2 diabetes at a tertiary academic medical center and increase a baseline screening rate of 56%-75% over 6 months (September 2022-February 2023) and sustain that increase for 6 months (March through August 2023).
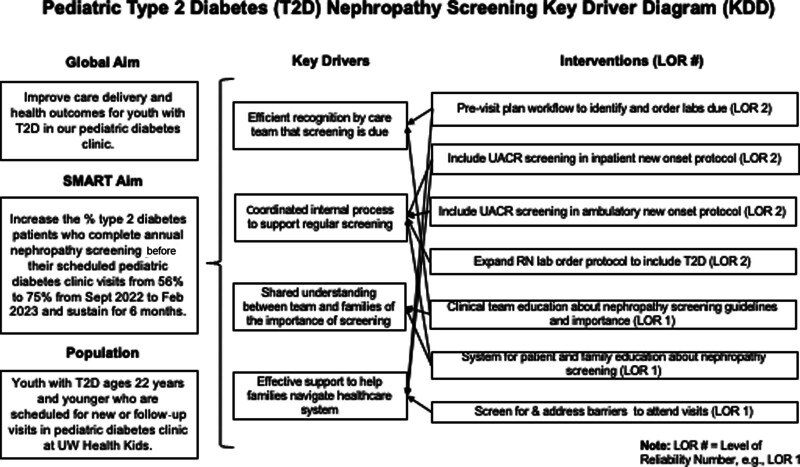
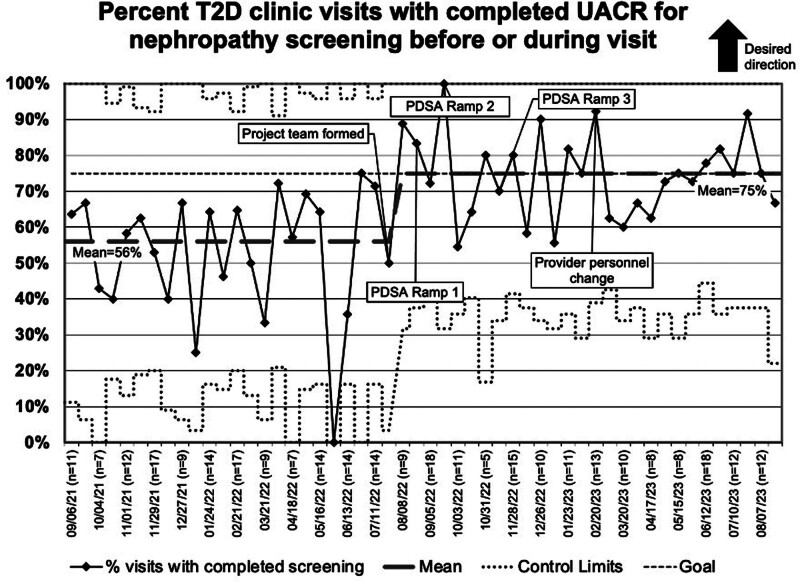
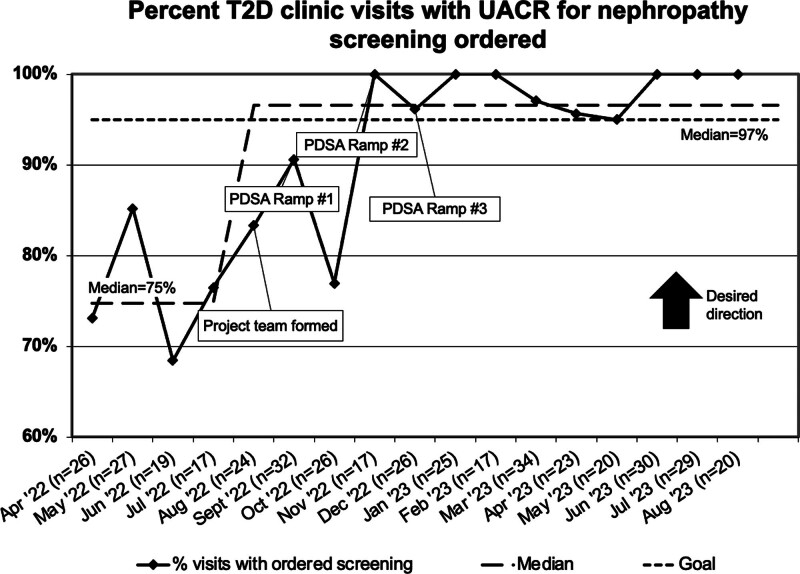
Methods: A multi-disciplinary team used quality improvement methods and iterative Plan-Do-Study-Act cycles. Targeted interventions included previsit planning workflow, education, and a new-onset triage protocol. The team collected data at baseline and prospectively by reviewing electronic medical records. The primary outcome measure was pediatric type 2 diabetes clinic visits in diabetes clinic with urine nephropathy screening before or on the visit date.
Results: A total of 121 youth were scheduled for T2D clinic visits between September 2021 and August 2023. The mean age was 14.5 years, and 60% were women, 40% were non-Hispanic Black, 28% were Hispanic/Latino, and 15% reported Spanish as their preferred language. Following the interventions of this project, urine nephropathy screening increased from 56% to 75%, and this change was sustained for 6 months.
Conclusions: Interventions focused on efficient recognition of the population needing screening, coordinated internal processes around screening, a shared understanding between all stakeholders, and practical support in the healthcare system increased urine nephropathy screening with sustained improvement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


