Amanda S Dupont, Patrick C Drayna, Mark Nimmer, Shannon H Baumer-Mouradian, Kendra Wirkus, Danny G Thomas, Kevin Boyd, Sri S Chinta
{"title":"Improving Turnaround Time of Transabdominal Pelvic Ultrasounds with Ovarian Doppler in a Pediatric Emergency Department.","authors":"Amanda S Dupont, Patrick C Drayna, Mark Nimmer, Shannon H Baumer-Mouradian, Kendra Wirkus, Danny G Thomas, Kevin Boyd, Sri S Chinta","doi":"10.1097/pq9.0000000000000730","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Adnexal torsion is an emergent surgical condition. Transabdominal pelvic ultrasound (US) with ovarian Doppler is used to diagnose adnexal torsion and requires a sufficient bladder volume. Reduce the turnaround time for US by 25% in girls 8-18 years of age who present to the emergency department (ED) for 24 months.</p><p><strong>Methods: </strong>Our baseline period was from January 2020 to June 2021, and the intervention period was from July 2021 to June 2023. Patients 8-18 years old who required an US in the ED were included. There are two key drivers: early identification of US readiness and expeditious bladder filling. Interventions were (1) bladder volume screening; (2) utilization of bladder volume nomogram to identify US readiness; (3) epic order panels; and (4) rapid intravenous fluid method. The primary outcome was US turnaround time. Secondary outcomes were percentage of patients requiring invasive interventions to fill the bladder and patients with an US study duration of ≤45 minutes. The percent of patients screened by bladder scan was used as a process measure. Balancing measures used episodes of fluid overload and ED length of stay.</p><p><strong>Results: </strong>Turnaround time for USs improved from 112.4 to 101.6 minutes. The percentage of patients who had successful USs without invasive bladder filling improved from 32.1% to 42.6%. Bladder volume screening using a bladder scan increased from 40.3% to 82.9%. The successful first-pass US completion rate improved from 77% to 90% consistently.</p><p><strong>Conclusions: </strong>Through quality improvement methodology, we have identified pelvic US readiness earlier, eliminated some invasive bladder-filling measures, and implemented a rapid fluid protocol. We have sustained these successful results for 2 years. This study can be generalized to any ED with similar patients.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e730"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11132411/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000730","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Adnexal torsion is an emergent surgical condition. Transabdominal pelvic ultrasound (US) with ovarian Doppler is used to diagnose adnexal torsion and requires a sufficient bladder volume. Reduce the turnaround time for US by 25% in girls 8-18 years of age who present to the emergency department (ED) for 24 months.
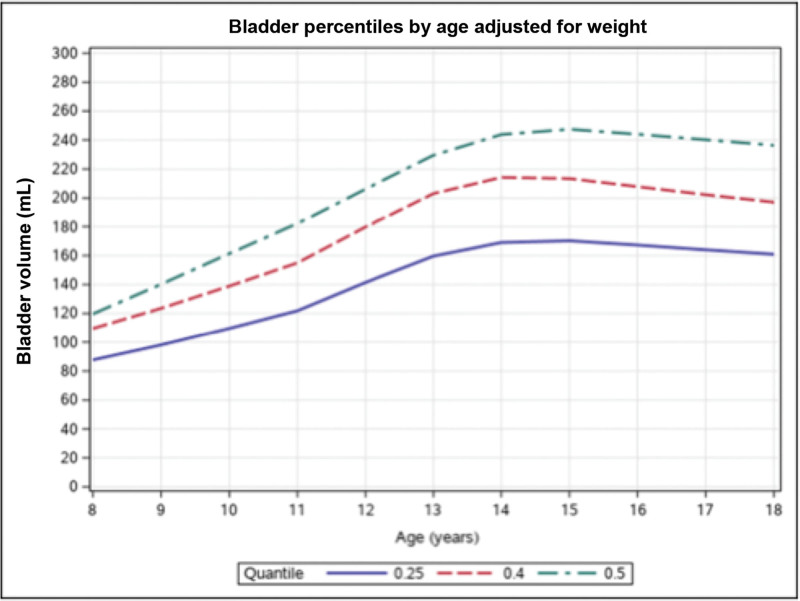
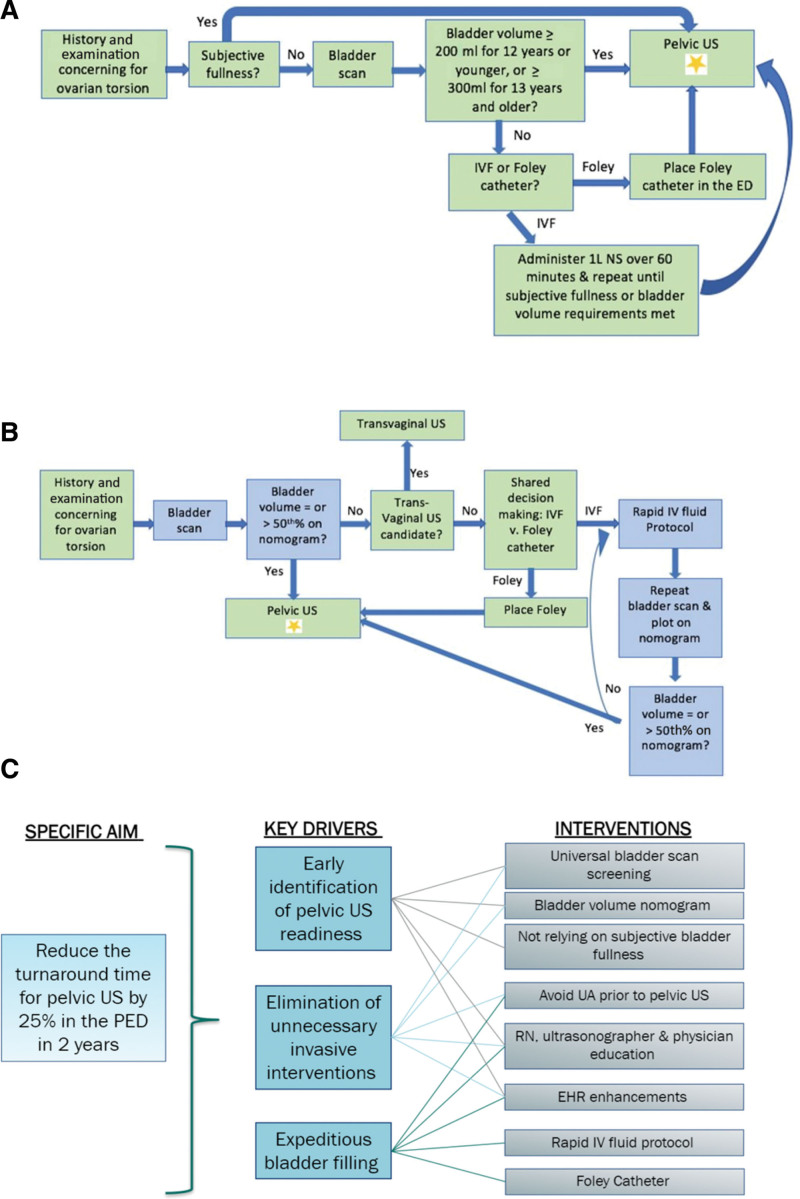
Methods: Our baseline period was from January 2020 to June 2021, and the intervention period was from July 2021 to June 2023. Patients 8-18 years old who required an US in the ED were included. There are two key drivers: early identification of US readiness and expeditious bladder filling. Interventions were (1) bladder volume screening; (2) utilization of bladder volume nomogram to identify US readiness; (3) epic order panels; and (4) rapid intravenous fluid method. The primary outcome was US turnaround time. Secondary outcomes were percentage of patients requiring invasive interventions to fill the bladder and patients with an US study duration of ≤45 minutes. The percent of patients screened by bladder scan was used as a process measure. Balancing measures used episodes of fluid overload and ED length of stay.
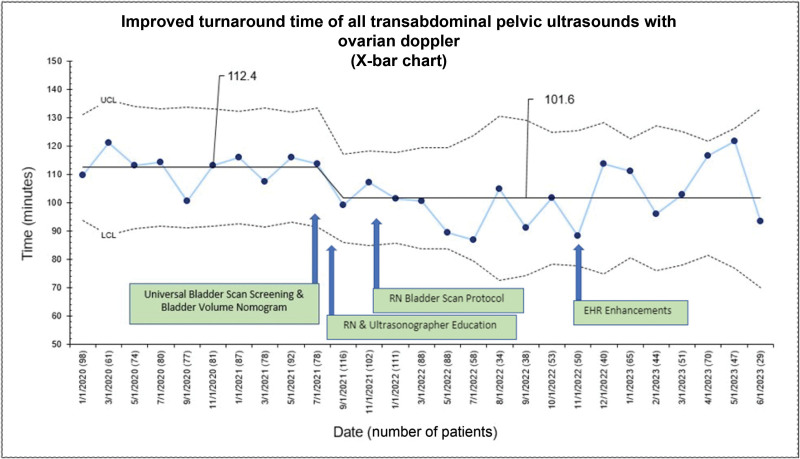
Results: Turnaround time for USs improved from 112.4 to 101.6 minutes. The percentage of patients who had successful USs without invasive bladder filling improved from 32.1% to 42.6%. Bladder volume screening using a bladder scan increased from 40.3% to 82.9%. The successful first-pass US completion rate improved from 77% to 90% consistently.
Conclusions: Through quality improvement methodology, we have identified pelvic US readiness earlier, eliminated some invasive bladder-filling measures, and implemented a rapid fluid protocol. We have sustained these successful results for 2 years. This study can be generalized to any ED with similar patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


