Diagnostic accuracy of morning serum cortisol concentration in confirming recovery of the hypothalamic-pituitary-adrenal axis in patients on chronic glucocorticoid therapy
Ella Sharma, Joe Berry, Bridget Griffiths, Alice Lorenzi, Ben Thompson, Chris Boot, Yaasir Mamoojee
{"title":"Diagnostic accuracy of morning serum cortisol concentration in confirming recovery of the hypothalamic-pituitary-adrenal axis in patients on chronic glucocorticoid therapy","authors":"Ella Sharma, Joe Berry, Bridget Griffiths, Alice Lorenzi, Ben Thompson, Chris Boot, Yaasir Mamoojee","doi":"10.1111/cen.15077","DOIUrl":null,"url":null,"abstract":"<p>Chronic glucocorticoid therapy (CGT) is widely used in a variety of medical specialities as an anti-inflammatory and immunosuppressive agent. The prevalence of oral CGT use can be as high as 3% in some populations, and as such CGT above physiological dosing and for a prolonged period of time invariably carries an increased risk of glucocorticoid-induced adrenal insufficiency (AI). In clinical practice, the oral dose of CGT is gradually reduced according to disease activity and to prevent flare, as well as allowing for recovery of the hypothalamic–pituitary–adrenal (HPA) axis.<span><sup>1</sup></span> Many centres undertake inappropriate 250 µg Synacthen tests (SST) in patients who may be on suppressive doses of prednisolone, especially those suffering from hypo-adrenal symptoms on tapering steroid doses (arthralgia/myalgia, lethargy, weakness, sleep disturbance and mood changes).</p><p>We previously reported that an early morning serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) on the Cortisol-II assay (by Roche Diagnostics) has 100% specificity at confirming an intact HPA axis in a large cohort of patients at risk of secondary AI from pituitary disease.<span><sup>2</sup></span> Given that the pathophysiology of AI in CGT and pituitary disease is comparable and secondary to low/suppressed secretion of adrenocorticotropic hormone from the pituitary gland, we postulated that the same morning serum cortisol concentration cutoff can be applied as a screening test for patients on CGT. To validate this cutoff, we retrospectively reviewed SST results performed in patients on tapering doses of CGT, from our rheumatology department, over a 12-month period. This study was registered as a service evaluation within our institution.</p><p>All SSTs were performed in the morning (7 AM to 12 AM) after withholding CGT for 48 h. Peripheral blood was sampled for cortisol at baseline, 30 and 60 min. AI was defined as a peak serum cortisol concentration <420 nmol/L (<15.2 μg/dL) (Cortisol-II assay Roche Diagnostics), based on previously validated cutoff values from healthy control population.<span><sup>3</sup></span> Data is expressed as mean (±SD) and percentages. Mann–Whitney test was used for statistical analyses between continuous variables.</p><p>Sixty SSTs were performed on 58 patients. The mean age of our cohort was 65( ± 15) years with a female predominance of 2:1. Mean duration of CGT was 63( ± 42) months, prescribed primarily for giant cell arteritis/polymyalgia rheumatica (48%) and inflammatory arthritis (18%). All patients were on prednisolone as CGT and the mean daily dose was 3.4 (±2.5) mg at the time of SST. 15% of our cohort had a failed SST. With our previously reported basal serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) used to confirm an intact HPA axis, no patient with AI would have been missed, but 37 out of 51 (73%) unnecessary SSTs in euadrenal patients would have been avoided. Receiver operating curve analysis (see Supporting Information Appendix) demonstrates a basal serum cortisol concentration of >227 nmol/L had a specificity of 100% for predicting passing the SST, while a basal serum cortisol concentration of ≤55 nmol/L had a 100% sensitivity for predicting failure (area under the curve: 0.916, 95% confidence interval: 0.815–0.972).</p><p>Notably, mean daily prednisolone dosing at time of SST in patients with AI was significantly higher than those with normal SSTs (5.7 mg vs. 2.9 mg respectively, <i>p</i> = .01). Figure 1 illustrates the distribution of daily prednisolone dosing between the two groups.</p><p>Sagar et al. previously reported that 100% of patients on chronic CGT with a morning cortisol <100 nmol/L (<3.6 μg/dL) on ADVIA Centaur cortisol immunoassay (Siemens) had a failed SST, while all patients with morning cortisol >350 nmol/L (>12.6 μg/dL) had a clear pass.<span><sup>4</sup></span> Additionally, Sbardella et al. demonstrated that a morning cortisol ≥336 nmol/L (≥12.1 μg/dL) on Abbott Architect i-2000 immunoassay had a specificity of 100% for predicting a normal SST, and morning cortisol ≤83 nmol/L (≤3 μg/dL) was 100% sensitive for AI.<span><sup>5</sup></span> It is worth noting that a minority of patients were prescribed CGT for non-endocrine conditions in the latter cohort.</p><p>Our data validates a morning serum cortisol concentration of >237 nmol/L (>8.6 μg/dL), on the Cortisol-II assay by Roche Diagnostics, with 100% specificity at predicting recovery of HPA axis in patients on tapering doses of CGT. This offers a more rapid, convenient and cost-effective screening method for patients requiring biochemical assessment of the HPA axis with the potential for significant resource savings without any adverse impact on patient safety. In most centres, the treatment of GCA involves prednisolone reduction very successfully, without the involvement of endocrinologists, for example, by reducing the dose over a few weeks from 60 to 10 mg, and then reducing the dose by 1 mg per month. The involvement of endocrinologists potentially limits the ability of the rheumatologists to wean the patient off prednisolone independently and should therefore not be the norm. Our observation further empowers the rheumatologists to wean patients off prednisolone safely, thus reversing the trend of endocrinology involvement.</p><p>Our data further suggest that assessment of the HPA axis, if desired during tapering doses of CGT, should be considered once a daily prednisolone dose of ≤3 mg is reached. This is consistent with a recent study demonstrating that a once-daily prednisolone dose of 2–4 mg is more physiological based on achieving serum prednisolone concentrations within therapeutic target ranges in patients with AI.<span><sup>6</sup></span> It is assumed by many that prednisolone 5 mg once daily is not a suppressive dose and, indeed in many countries, the lowest strength tablet available is 5 mg. Therefore, in the absence of intercurrent acute illnesses, patients experiencing presumed hypoadrenal symptoms on a supra-therapeutic daily prednisolone dose of >4 mg may be considered to have steroid withdrawal symptoms. As such avoiding biochemical assessment to evaluate the integrity of the HPA axis in such patients but slowing down the rate of glucocorticoid tapering instead would be a clinically sound strategy.</p><p>In summary, we have validated an early serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) as a safe and useful screening test with 100% specificity for predicting recovery of HPA axis in patients on long-term CGT on tapering regimes (although it should be noted that morning serum cortisol screening cutoff thresholds may vary depending on the assay utilised for cortisol measurements). Clinicians need to re-evaluate the utility of any endocrine testing in rheumatology patients who are being weaned, as patients who have a low morning cortisol or a failed SST only do so because of the prednisolone, and the only way to recover the axis is to reduce the suppressive steroid further. Nevertheless, clinicians may contemplate biochemical assessment of HPA recovery, if necessary, once a daily prednisolone dose of ≤3 mg is reached during the steroid tapering process.</p>","PeriodicalId":10346,"journal":{"name":"Clinical Endocrinology","volume":null,"pages":null},"PeriodicalIF":3.0000,"publicationDate":"2024-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen.15077","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cen.15077","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Chronic glucocorticoid therapy (CGT) is widely used in a variety of medical specialities as an anti-inflammatory and immunosuppressive agent. The prevalence of oral CGT use can be as high as 3% in some populations, and as such CGT above physiological dosing and for a prolonged period of time invariably carries an increased risk of glucocorticoid-induced adrenal insufficiency (AI). In clinical practice, the oral dose of CGT is gradually reduced according to disease activity and to prevent flare, as well as allowing for recovery of the hypothalamic–pituitary–adrenal (HPA) axis.1 Many centres undertake inappropriate 250 µg Synacthen tests (SST) in patients who may be on suppressive doses of prednisolone, especially those suffering from hypo-adrenal symptoms on tapering steroid doses (arthralgia/myalgia, lethargy, weakness, sleep disturbance and mood changes).
We previously reported that an early morning serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) on the Cortisol-II assay (by Roche Diagnostics) has 100% specificity at confirming an intact HPA axis in a large cohort of patients at risk of secondary AI from pituitary disease.2 Given that the pathophysiology of AI in CGT and pituitary disease is comparable and secondary to low/suppressed secretion of adrenocorticotropic hormone from the pituitary gland, we postulated that the same morning serum cortisol concentration cutoff can be applied as a screening test for patients on CGT. To validate this cutoff, we retrospectively reviewed SST results performed in patients on tapering doses of CGT, from our rheumatology department, over a 12-month period. This study was registered as a service evaluation within our institution.
All SSTs were performed in the morning (7 AM to 12 AM) after withholding CGT for 48 h. Peripheral blood was sampled for cortisol at baseline, 30 and 60 min. AI was defined as a peak serum cortisol concentration <420 nmol/L (<15.2 μg/dL) (Cortisol-II assay Roche Diagnostics), based on previously validated cutoff values from healthy control population.3 Data is expressed as mean (±SD) and percentages. Mann–Whitney test was used for statistical analyses between continuous variables.
Sixty SSTs were performed on 58 patients. The mean age of our cohort was 65( ± 15) years with a female predominance of 2:1. Mean duration of CGT was 63( ± 42) months, prescribed primarily for giant cell arteritis/polymyalgia rheumatica (48%) and inflammatory arthritis (18%). All patients were on prednisolone as CGT and the mean daily dose was 3.4 (±2.5) mg at the time of SST. 15% of our cohort had a failed SST. With our previously reported basal serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) used to confirm an intact HPA axis, no patient with AI would have been missed, but 37 out of 51 (73%) unnecessary SSTs in euadrenal patients would have been avoided. Receiver operating curve analysis (see Supporting Information Appendix) demonstrates a basal serum cortisol concentration of >227 nmol/L had a specificity of 100% for predicting passing the SST, while a basal serum cortisol concentration of ≤55 nmol/L had a 100% sensitivity for predicting failure (area under the curve: 0.916, 95% confidence interval: 0.815–0.972).
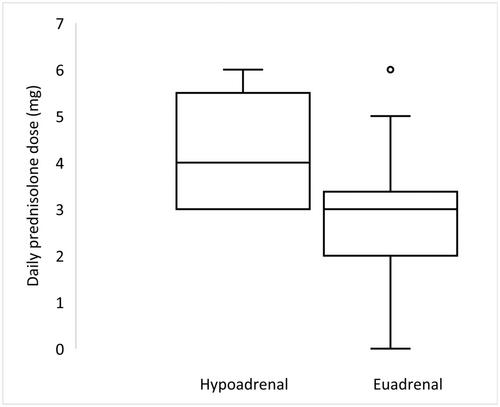
Notably, mean daily prednisolone dosing at time of SST in patients with AI was significantly higher than those with normal SSTs (5.7 mg vs. 2.9 mg respectively, p = .01). Figure 1 illustrates the distribution of daily prednisolone dosing between the two groups.
Sagar et al. previously reported that 100% of patients on chronic CGT with a morning cortisol <100 nmol/L (<3.6 μg/dL) on ADVIA Centaur cortisol immunoassay (Siemens) had a failed SST, while all patients with morning cortisol >350 nmol/L (>12.6 μg/dL) had a clear pass.4 Additionally, Sbardella et al. demonstrated that a morning cortisol ≥336 nmol/L (≥12.1 μg/dL) on Abbott Architect i-2000 immunoassay had a specificity of 100% for predicting a normal SST, and morning cortisol ≤83 nmol/L (≤3 μg/dL) was 100% sensitive for AI.5 It is worth noting that a minority of patients were prescribed CGT for non-endocrine conditions in the latter cohort.
Our data validates a morning serum cortisol concentration of >237 nmol/L (>8.6 μg/dL), on the Cortisol-II assay by Roche Diagnostics, with 100% specificity at predicting recovery of HPA axis in patients on tapering doses of CGT. This offers a more rapid, convenient and cost-effective screening method for patients requiring biochemical assessment of the HPA axis with the potential for significant resource savings without any adverse impact on patient safety. In most centres, the treatment of GCA involves prednisolone reduction very successfully, without the involvement of endocrinologists, for example, by reducing the dose over a few weeks from 60 to 10 mg, and then reducing the dose by 1 mg per month. The involvement of endocrinologists potentially limits the ability of the rheumatologists to wean the patient off prednisolone independently and should therefore not be the norm. Our observation further empowers the rheumatologists to wean patients off prednisolone safely, thus reversing the trend of endocrinology involvement.
Our data further suggest that assessment of the HPA axis, if desired during tapering doses of CGT, should be considered once a daily prednisolone dose of ≤3 mg is reached. This is consistent with a recent study demonstrating that a once-daily prednisolone dose of 2–4 mg is more physiological based on achieving serum prednisolone concentrations within therapeutic target ranges in patients with AI.6 It is assumed by many that prednisolone 5 mg once daily is not a suppressive dose and, indeed in many countries, the lowest strength tablet available is 5 mg. Therefore, in the absence of intercurrent acute illnesses, patients experiencing presumed hypoadrenal symptoms on a supra-therapeutic daily prednisolone dose of >4 mg may be considered to have steroid withdrawal symptoms. As such avoiding biochemical assessment to evaluate the integrity of the HPA axis in such patients but slowing down the rate of glucocorticoid tapering instead would be a clinically sound strategy.
In summary, we have validated an early serum cortisol concentration of >237 nmol/L (>8.6 μg/dL) as a safe and useful screening test with 100% specificity for predicting recovery of HPA axis in patients on long-term CGT on tapering regimes (although it should be noted that morning serum cortisol screening cutoff thresholds may vary depending on the assay utilised for cortisol measurements). Clinicians need to re-evaluate the utility of any endocrine testing in rheumatology patients who are being weaned, as patients who have a low morning cortisol or a failed SST only do so because of the prednisolone, and the only way to recover the axis is to reduce the suppressive steroid further. Nevertheless, clinicians may contemplate biochemical assessment of HPA recovery, if necessary, once a daily prednisolone dose of ≤3 mg is reached during the steroid tapering process.
期刊介绍:
Clinical Endocrinology publishes papers and reviews which focus on the clinical aspects of endocrinology, including the clinical application of molecular endocrinology. It does not publish papers relating directly to diabetes care and clinical management. It features reviews, original papers, commentaries, correspondence and Clinical Questions. Clinical Endocrinology is essential reading not only for those engaged in endocrinological research but also for those involved primarily in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


