Mary C McLellan, Mariam Irshad, Katherine C Penny, Michelle Rufo, Sarah Atwood, Heather Dacey, Christina M Ireland, Sarah de Ferranti, Theresa Saia, Anna C Fisk, Susan F Saleeb
{"title":"Enhanced Safety and Efficiency of Ambulatory Cardiology Admissions: A Quality Improvement Initiative.","authors":"Mary C McLellan, Mariam Irshad, Katherine C Penny, Michelle Rufo, Sarah Atwood, Heather Dacey, Christina M Ireland, Sarah de Ferranti, Theresa Saia, Anna C Fisk, Susan F Saleeb","doi":"10.1097/pq9.0000000000000726","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pediatric cardiac patients have experienced evolving illnesses progressing to instability while awaiting inpatient admission from ambulatory settings. Admission delays and communication breakdowns increase the risk for tenuous patients. This quality improvement initiative aimed to improve safety and efficiency for patients admitted from an ambulatory Clinic to the Acute Cardiac Care Unit (ACCU) using standardized communication and admission processes within one year.</p><p><strong>Methods: </strong>An admission process map, in-clinic nurse monitoring, and communication pathways were developed and implemented. A standardized team handoff occurred via virtual huddle using illness severity, patient summary, action list, situational awareness, and synthesis. Escalation of care events and timeliness were compared pre- and postimplementation.</p><p><strong>Results: </strong>There was a reduction of transfers to the intensive care unit within 24 hours of ACCU admission from 9.2% to 3.8% (<i>P</i> = 0.26), intensive care unit evaluations (without transfer) from 5.6% to 0% (<i>P</i> = 0.06), and arrests from 3.7% to 0% (<i>P</i> = 0.16). After the pilot, clinic nurses monitored 100% of at-risk patients. Overall mean time from admission decision to virtual huddle decreased from 81 to 61 minutes and mean time to admission from 144 to 115 minutes, with 41% (n = 33) arriving ≤ 60 minutes (goal). The COVID-19 pandemic negatively affected admission timeliness while safety metrics remained optimized.</p><p><strong>Conclusions: </strong>Implementing a standardized admission process between the Clinic and ACCU enhanced safety by reducing admission wait time and escalation of care post-admission. Sustainable, reliable handoff processes, in-clinic monitoring, and standardized admission processes were established. The pandemic hindered admission efficiency without compromising safety.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e726"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093579/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000726","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
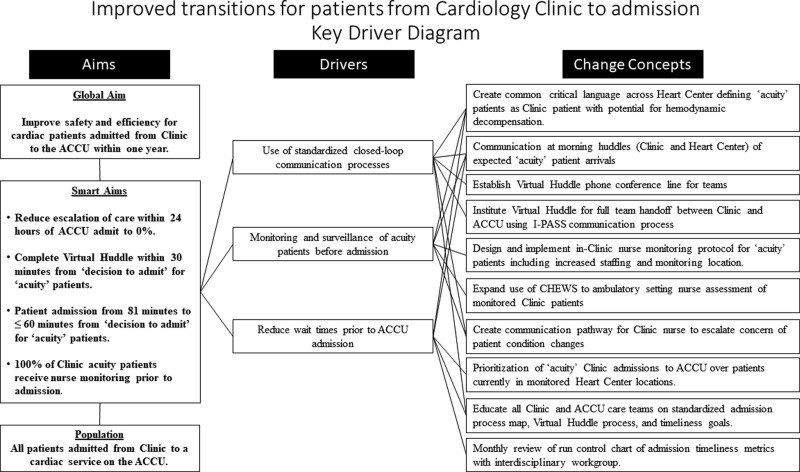
Background: Pediatric cardiac patients have experienced evolving illnesses progressing to instability while awaiting inpatient admission from ambulatory settings. Admission delays and communication breakdowns increase the risk for tenuous patients. This quality improvement initiative aimed to improve safety and efficiency for patients admitted from an ambulatory Clinic to the Acute Cardiac Care Unit (ACCU) using standardized communication and admission processes within one year.
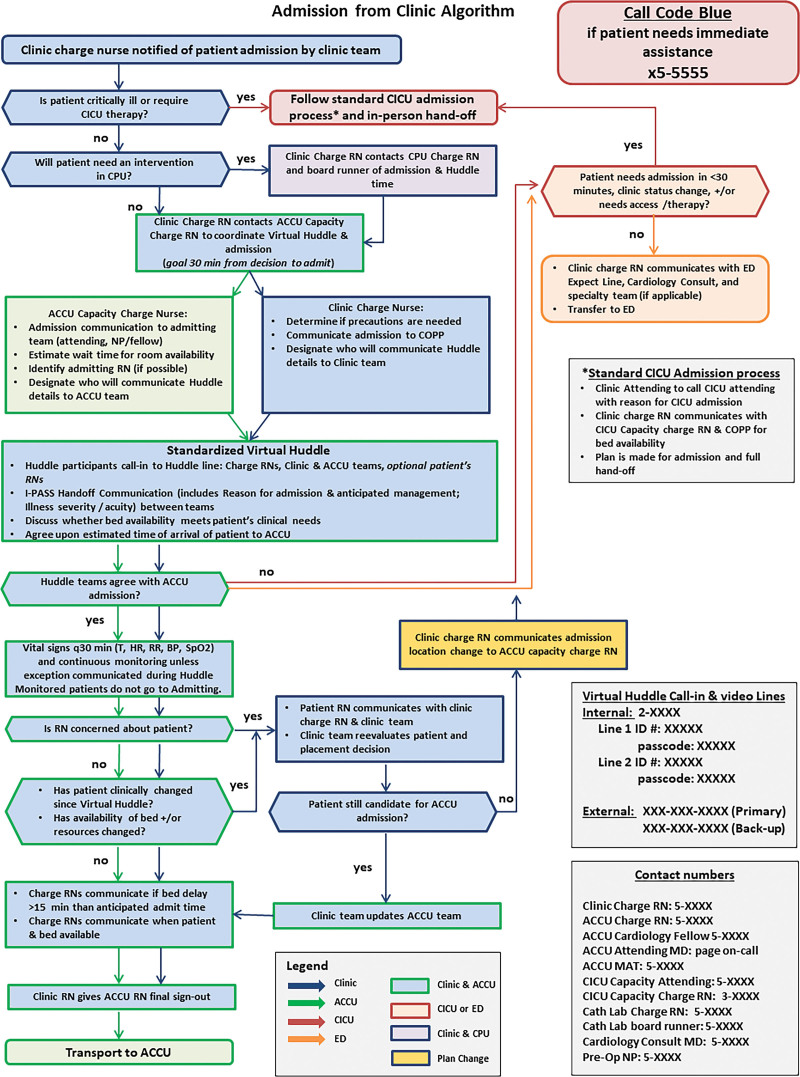
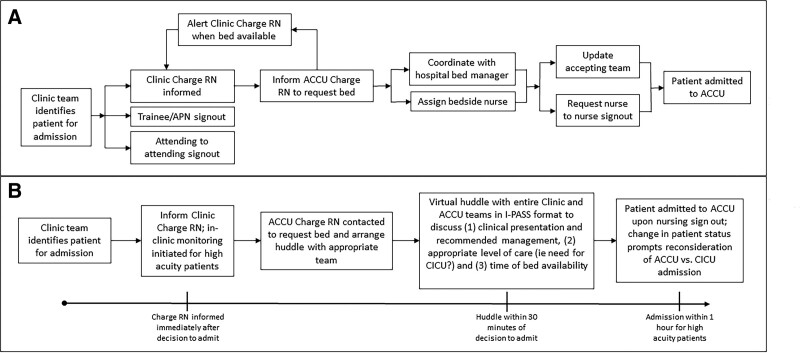
Methods: An admission process map, in-clinic nurse monitoring, and communication pathways were developed and implemented. A standardized team handoff occurred via virtual huddle using illness severity, patient summary, action list, situational awareness, and synthesis. Escalation of care events and timeliness were compared pre- and postimplementation.
Results: There was a reduction of transfers to the intensive care unit within 24 hours of ACCU admission from 9.2% to 3.8% (P = 0.26), intensive care unit evaluations (without transfer) from 5.6% to 0% (P = 0.06), and arrests from 3.7% to 0% (P = 0.16). After the pilot, clinic nurses monitored 100% of at-risk patients. Overall mean time from admission decision to virtual huddle decreased from 81 to 61 minutes and mean time to admission from 144 to 115 minutes, with 41% (n = 33) arriving ≤ 60 minutes (goal). The COVID-19 pandemic negatively affected admission timeliness while safety metrics remained optimized.
Conclusions: Implementing a standardized admission process between the Clinic and ACCU enhanced safety by reducing admission wait time and escalation of care post-admission. Sustainable, reliable handoff processes, in-clinic monitoring, and standardized admission processes were established. The pandemic hindered admission efficiency without compromising safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


