Emma Christensen, Helge Fagerheim Bugge, Jostein Hagemo, Karianne Larsen, Astrid Kv Harring, Jostein Gleditsch, Jørgen Ibsen, Mona Guterud, Else Charlotte Sandset, Maren Ranhoff Hov
{"title":"Prehospital stroke diagnostics using three different simulation methods: A pragmatic pilot study.","authors":"Emma Christensen, Helge Fagerheim Bugge, Jostein Hagemo, Karianne Larsen, Astrid Kv Harring, Jostein Gleditsch, Jørgen Ibsen, Mona Guterud, Else Charlotte Sandset, Maren Ranhoff Hov","doi":"10.1177/23969873241252564","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The optimal pathway for ultra-early diagnostics and treatment in patients with acute stroke remains uncertain. The aim of this study was to investigate how three different methods of simulated, rural prehospital computed tomography (CT) affected the time to prehospital treatment decision in acute stroke.</p><p><strong>Materials and methods: </strong>In this pragmatic, simulation, pilot study of prehospital CT we investigated a conventional ambulance with transport to a standard care rural stationary CT machine managed by paramedics, a Mobile Stroke Unit (MSU), and a helicopter with a simulated CT machine. Each modality completed 20 real-life dispatches combined with simulation of predetermined animated patient cases with acute stroke symptoms and CT images. The primary endpoint of the study was the time from alarm to treatment decision.</p><p><strong>Results: </strong>Median time from alarm to the treatment decision differed significantly between the three groups (<i>p</i> = 0.0005), with 38 min for rural CT, 33 min for the MSU, and 30 min for the helicopter. There was no difference in time when comparing rural CT with MSU, nor when comparing the MSU with the helicopter. There was a difference in time to treatment decision between the rural CT and the helicopter (<i>p</i> < 0.0001). The helicopter had significantly lower estimated time from treatment decision to hospital (<i>p</i> = 0.001).</p><p><strong>Disscussion/conclusion: </strong>Prehospital CT can be organized in several ways depending on geography, resources and need. Further research on paramedic run rural CT, MSU in rural areas, and helicopter CT is needed to find the optimal strategy.</p>","PeriodicalId":46821,"journal":{"name":"European Stroke Journal","volume":" ","pages":"1016-1024"},"PeriodicalIF":4.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11569525/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Stroke Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23969873241252564","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The optimal pathway for ultra-early diagnostics and treatment in patients with acute stroke remains uncertain. The aim of this study was to investigate how three different methods of simulated, rural prehospital computed tomography (CT) affected the time to prehospital treatment decision in acute stroke.
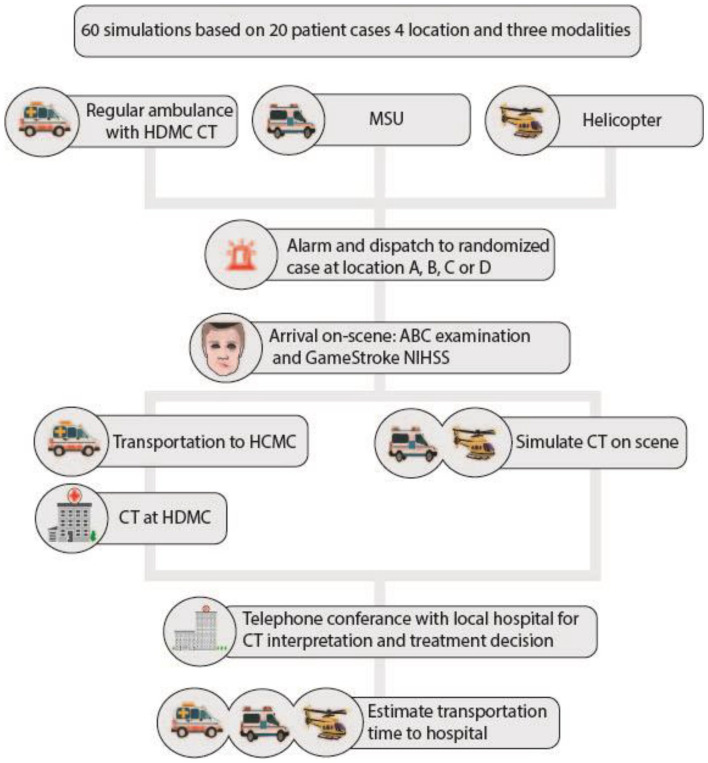
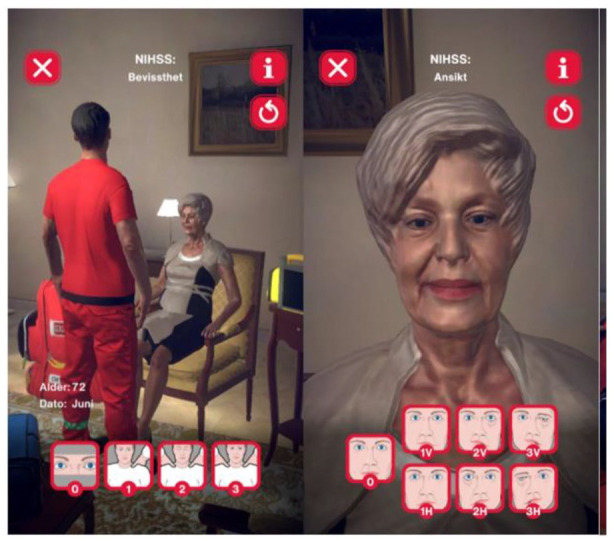
Materials and methods: In this pragmatic, simulation, pilot study of prehospital CT we investigated a conventional ambulance with transport to a standard care rural stationary CT machine managed by paramedics, a Mobile Stroke Unit (MSU), and a helicopter with a simulated CT machine. Each modality completed 20 real-life dispatches combined with simulation of predetermined animated patient cases with acute stroke symptoms and CT images. The primary endpoint of the study was the time from alarm to treatment decision.
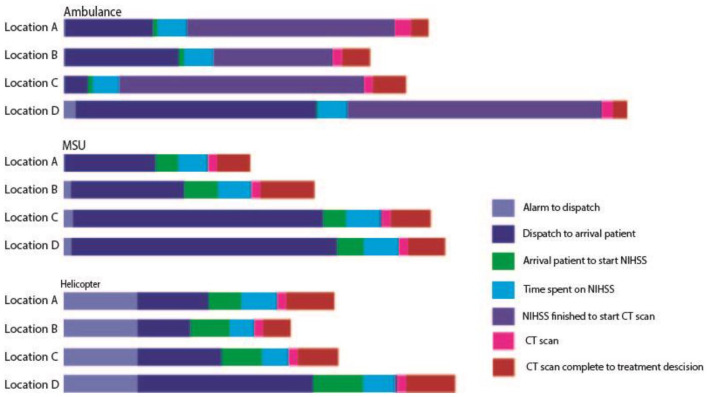
Results: Median time from alarm to the treatment decision differed significantly between the three groups (p = 0.0005), with 38 min for rural CT, 33 min for the MSU, and 30 min for the helicopter. There was no difference in time when comparing rural CT with MSU, nor when comparing the MSU with the helicopter. There was a difference in time to treatment decision between the rural CT and the helicopter (p < 0.0001). The helicopter had significantly lower estimated time from treatment decision to hospital (p = 0.001).
Disscussion/conclusion: Prehospital CT can be organized in several ways depending on geography, resources and need. Further research on paramedic run rural CT, MSU in rural areas, and helicopter CT is needed to find the optimal strategy.
期刊介绍:
Launched in 2016 the European Stroke Journal (ESJ) is the official journal of the European Stroke Organisation (ESO), a professional non-profit organization with over 1,400 individual members, and affiliations to numerous related national and international societies. ESJ covers clinical stroke research from all fields, including clinical trials, epidemiology, primary and secondary prevention, diagnosis, acute and post-acute management, guidelines, translation of experimental findings into clinical practice, rehabilitation, organisation of stroke care, and societal impact. It is open to authors from all relevant medical and health professions. Article types include review articles, original research, protocols, guidelines, editorials and letters to the Editor. Through ESJ, authors and researchers have gained a new platform for the rapid and professional publication of peer reviewed scientific material of the highest standards; publication in ESJ is highly competitive. The journal and its editorial team has developed excellent cooperation with sister organisations such as the World Stroke Organisation and the International Journal of Stroke, and the American Heart Organization/American Stroke Association and the journal Stroke. ESJ is fully peer-reviewed and is a member of the Committee on Publication Ethics (COPE). Issues are published 4 times a year (March, June, September and December) and articles are published OnlineFirst prior to issue publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


