Practical application of the modification in endoscopic retrograde cholangiopancreatography treated common bile duct stones in patients with Billroth II gastroenterostomy in Vietnam.
Tran Thi Anh Tuyet, Nguyen Van Thai, Nguyen Tien Thinh, Mai Thanh Binh
{"title":"Practical application of the modification in endoscopic retrograde cholangiopancreatography treated common bile duct stones in patients with Billroth II gastroenterostomy in Vietnam.","authors":"Tran Thi Anh Tuyet, Nguyen Van Thai, Nguyen Tien Thinh, Mai Thanh Binh","doi":"10.1177/26317745241251713","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) in patients who have undergone Billroth II gastroenterostomy (B-II GE) has been challenging, requiring flexibility in technical approaches during execution. The study aims to assess the effectiveness of enhanced techniques in performing ERCP on this patient group in Vietnam.</p><p><strong>Method: </strong>A total of 42 Vietnamese patients with B-II GE performed an ERCP using a duodenoscope or a modification of ERCP equipment (a cap-fitted regular forward-viewing endoscope) if the former failed. The effectiveness and safety of the ERCP technique were assessed, particularly in patients who underwent the forward-viewing endoscope method.</p><p><strong>Result: </strong>A total of 39 out of 42 patients had the Vater's papilla identified, among whom 12 patients (30.8%) achieved successful cannulation into the bile duct using a side-viewing endoscope, significantly lower than the success rate using a forward-viewing endoscope (25/27, counted 92.6%, with <i>p</i> < 0.001). After successful cannulation, the rate of stone clearance, the procedural time, and the hospitalization duration of the patients were equivalent between the two methods and were not dependent on the number or size of the stones. On the other hand, post-ERCP complications in patients utilizing forward-viewing endoscopy included acute pancreatitis (22.2%), post-sphincterotomy bleeding (3.7%), septicemia (4.8%), and perforation (0%). These complications were mild and amenable to conservative endoscopic and medical management, and no mortality was observed. The rates of complications and adverse events after ERCP are comparable between the two treatment methods, even though the end-viewing endoscope is used after the failure of the side-viewing endoscope.</p><p><strong>Conclusion: </strong>Alter ERCP utilizing a cap-fitted forward-viewing endoscope can be a primary choice for treating common bile duct stones in patients with a Billroth II gastric resection history because of high efficacy and acceptable complications. It requires a high level of procedural expertise that requires multiple training sessions.</p>","PeriodicalId":40947,"journal":{"name":"Therapeutic Advances in Gastrointestinal Endoscopy","volume":"17 ","pages":"26317745241251713"},"PeriodicalIF":2.4000,"publicationDate":"2024-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11092305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastrointestinal Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26317745241251713","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Endoscopic retrograde cholangiopancreatography (ERCP) in patients who have undergone Billroth II gastroenterostomy (B-II GE) has been challenging, requiring flexibility in technical approaches during execution. The study aims to assess the effectiveness of enhanced techniques in performing ERCP on this patient group in Vietnam.
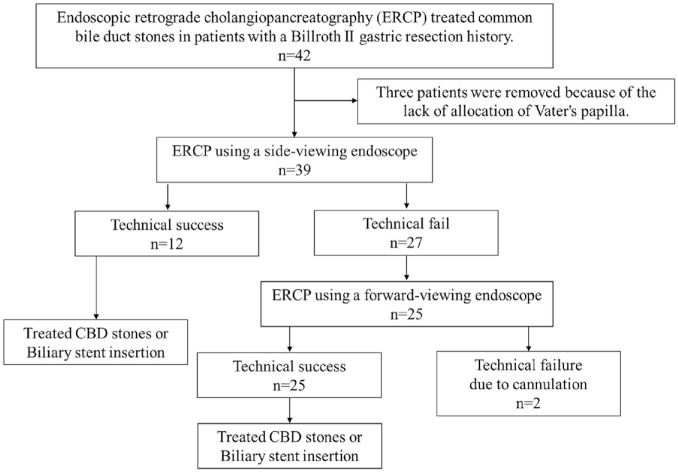
Method: A total of 42 Vietnamese patients with B-II GE performed an ERCP using a duodenoscope or a modification of ERCP equipment (a cap-fitted regular forward-viewing endoscope) if the former failed. The effectiveness and safety of the ERCP technique were assessed, particularly in patients who underwent the forward-viewing endoscope method.
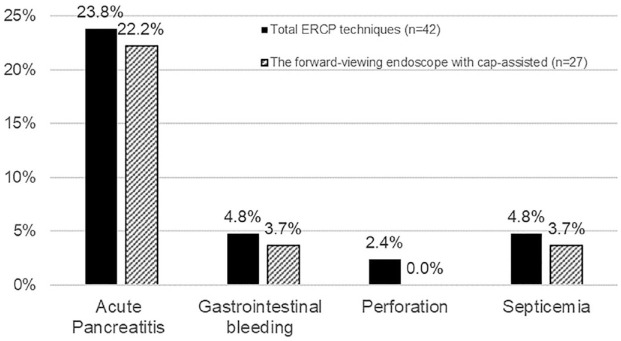
Result: A total of 39 out of 42 patients had the Vater's papilla identified, among whom 12 patients (30.8%) achieved successful cannulation into the bile duct using a side-viewing endoscope, significantly lower than the success rate using a forward-viewing endoscope (25/27, counted 92.6%, with p < 0.001). After successful cannulation, the rate of stone clearance, the procedural time, and the hospitalization duration of the patients were equivalent between the two methods and were not dependent on the number or size of the stones. On the other hand, post-ERCP complications in patients utilizing forward-viewing endoscopy included acute pancreatitis (22.2%), post-sphincterotomy bleeding (3.7%), septicemia (4.8%), and perforation (0%). These complications were mild and amenable to conservative endoscopic and medical management, and no mortality was observed. The rates of complications and adverse events after ERCP are comparable between the two treatment methods, even though the end-viewing endoscope is used after the failure of the side-viewing endoscope.
Conclusion: Alter ERCP utilizing a cap-fitted forward-viewing endoscope can be a primary choice for treating common bile duct stones in patients with a Billroth II gastric resection history because of high efficacy and acceptable complications. It requires a high level of procedural expertise that requires multiple training sessions.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


