Samantha Harrison MS, Krystal Capers MPH, Guanqing Chen PhD, Ji T. Liu PharmD, Ameeka Pannu MD, Valerie Goodspeed MPH, Akiva Leibowitz MD, Somnath Bose MD, MPH, FASA
{"title":"New initiation of opioids, benzodiazepines and antipsychotics following hospitalization for COVID-19","authors":"Samantha Harrison MS, Krystal Capers MPH, Guanqing Chen PhD, Ji T. Liu PharmD, Ameeka Pannu MD, Valerie Goodspeed MPH, Akiva Leibowitz MD, Somnath Bose MD, MPH, FASA","doi":"10.1002/jhm.13408","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Patients newly initiated on opioids (OP), benzodiazepines (BZD), and antipsychotics (AP) during hospitalization are often prescribed these on discharge. Implications of this practice on outcomes remains unexplored.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>To explore the prevalence and risk factors of new initiation of select OP, BZD and AP among patients requiring in-patient stays. Test the hypothesis that new prescriptions are associated with higher odds of readmission or death within 28 days of discharge.</p>\n </section>\n \n <section>\n \n <h3> Design</h3>\n \n <p>Single center retrospective cohort study.</p>\n </section>\n \n <section>\n \n <h3> Setting and Participants</h3>\n \n <p>Patients admitted to a tertiary-level medical center with either a primary diagnosis of RT-PCR positive for COVID-19 or high index of clinical suspicion thereof.</p>\n </section>\n \n <section>\n \n <h3> Intervention</h3>\n \n <p>None.</p>\n </section>\n \n <section>\n \n <h3> Main Outcome and Measures</h3>\n \n <p>Exposure was the new initiation of select common OP, BZD, and AP which were continued on hospital discharge. Outcome was a composite of 28-day readmission or death following index admission. Multivariable logistic regression was used to assess patient mortality or readmission within 28 days of discharge associated with new prescriptions at discharge.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>1319 patients were included in the analysis. 11.3% (149/1319) were discharged with a new prescription of select OP, BZD, or AP either alone or in combination. OP (110/149) were most prescribed followed by BZD (41/149) and AP (22/149). After adjusting for unbalanced confounders, new prescriptions (adjusted odds ratio: 2.44, 95% confidence interval: 1.42–4.12; <i>p</i> = .001) were associated with readmission or death within 28 days of discharge. One in nine patients admitted with a diagnosis of COVID-19 or high clinical suspicion thereof were discharged with a new prescription of either OP, BZD or AP. New prescriptions were associated with higher odds of 28-day readmission or death. Strengthening medication reconciliation processes focused on these classes may reduce avoidable harm.</p>\n </section>\n </div>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"19 10","pages":"877-885"},"PeriodicalIF":2.4000,"publicationDate":"2024-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhm.13408","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
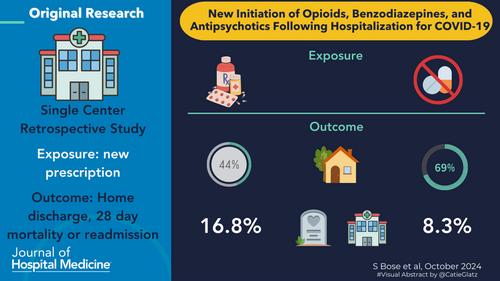
Patients newly initiated on opioids (OP), benzodiazepines (BZD), and antipsychotics (AP) during hospitalization are often prescribed these on discharge. Implications of this practice on outcomes remains unexplored.
Objective
To explore the prevalence and risk factors of new initiation of select OP, BZD and AP among patients requiring in-patient stays. Test the hypothesis that new prescriptions are associated with higher odds of readmission or death within 28 days of discharge.
Design
Single center retrospective cohort study.
Setting and Participants
Patients admitted to a tertiary-level medical center with either a primary diagnosis of RT-PCR positive for COVID-19 or high index of clinical suspicion thereof.
Intervention
None.
Main Outcome and Measures
Exposure was the new initiation of select common OP, BZD, and AP which were continued on hospital discharge. Outcome was a composite of 28-day readmission or death following index admission. Multivariable logistic regression was used to assess patient mortality or readmission within 28 days of discharge associated with new prescriptions at discharge.
Results
1319 patients were included in the analysis. 11.3% (149/1319) were discharged with a new prescription of select OP, BZD, or AP either alone or in combination. OP (110/149) were most prescribed followed by BZD (41/149) and AP (22/149). After adjusting for unbalanced confounders, new prescriptions (adjusted odds ratio: 2.44, 95% confidence interval: 1.42–4.12; p = .001) were associated with readmission or death within 28 days of discharge. One in nine patients admitted with a diagnosis of COVID-19 or high clinical suspicion thereof were discharged with a new prescription of either OP, BZD or AP. New prescriptions were associated with higher odds of 28-day readmission or death. Strengthening medication reconciliation processes focused on these classes may reduce avoidable harm.
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


