Ultrasound-guided suprainguinal fascia iliaca block to position the patient for neuraxial anaesthesia in acetabular surgery - a randomized controlled pilot study.
{"title":"Ultrasound-guided suprainguinal fascia iliaca block to position the patient for neuraxial anaesthesia in acetabular surgery - a randomized controlled pilot study.","authors":"Fathima Mohammed Ali, Arshad Ayub, Vanlal Darlong, Ravinder Kumar Pandey, Jyotsana Punj, Vijay Sharma","doi":"10.5114/ait.2024.138554","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Neuraxial anaesthesia is a common choice for most hip and lower limb operations. Pain associated with positioning is often a deterrent, and the vast literature suggests different regional blocks and opioids for these patients. Patients with acetabular fractures may experience increased pain, and thus are more difficult to position for the neuraxial block. We conducted a randomized controlled pilot study to assess and compare the analgesic efficacy of ultrasound-guided suprainguinal fascia iliaca block (SFICB) versus systemic fentanyl to facilitate positioning for combined spinal epidural (CSE) anaesthesia in patients undergoing acetabular fracture surgery.</p><p><strong>Material and methods: </strong>Twenty patients referred for surgical repair of acetabular fractures were randomly assigned to receive either ultrasound-guided SFICB (group B) or intravenous fentanyl (group F). Changes in visual analogue scale (VAS) scores in supine and sitting position, improvement in sitting angle (SA), positioning quality, rescue analgesic requirement, total opioid consumption, comfort VAS scores, and complications were noted to compare both groups.</p><p><strong>Results: </strong>The post-intervention VAS score in the sitting position was significantly lower in group B than in group F (5.9 ± 2.1 vs. 3.5 ± 1.5, P = 0.01). Group B also had more significant improvement in SA (27.5° (20.75-36.5°), in comparison to group F (10 (5-18.75), P = 0.006). The positioning quality was better in group B, with 70% of patients achieving an optimal position compared to only 10% in group F ( P = 0.02).</p><p><strong>Conclusions: </strong>Ultrasound-guided SFICB, as compared to systemic fentanyl, provided better analgesia and helped to achieve a better and more comfortable position to perform the neuraxial block.</p>","PeriodicalId":7750,"journal":{"name":"Anaesthesiology intensive therapy","volume":"56 1","pages":"54-60"},"PeriodicalIF":1.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11022634/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesiology intensive therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ait.2024.138554","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Neuraxial anaesthesia is a common choice for most hip and lower limb operations. Pain associated with positioning is often a deterrent, and the vast literature suggests different regional blocks and opioids for these patients. Patients with acetabular fractures may experience increased pain, and thus are more difficult to position for the neuraxial block. We conducted a randomized controlled pilot study to assess and compare the analgesic efficacy of ultrasound-guided suprainguinal fascia iliaca block (SFICB) versus systemic fentanyl to facilitate positioning for combined spinal epidural (CSE) anaesthesia in patients undergoing acetabular fracture surgery.
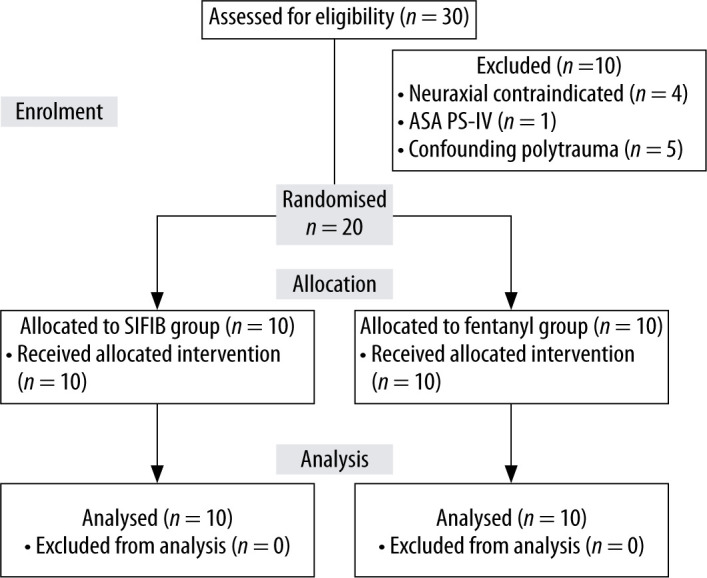
Material and methods: Twenty patients referred for surgical repair of acetabular fractures were randomly assigned to receive either ultrasound-guided SFICB (group B) or intravenous fentanyl (group F). Changes in visual analogue scale (VAS) scores in supine and sitting position, improvement in sitting angle (SA), positioning quality, rescue analgesic requirement, total opioid consumption, comfort VAS scores, and complications were noted to compare both groups.
Results: The post-intervention VAS score in the sitting position was significantly lower in group B than in group F (5.9 ± 2.1 vs. 3.5 ± 1.5, P = 0.01). Group B also had more significant improvement in SA (27.5° (20.75-36.5°), in comparison to group F (10 (5-18.75), P = 0.006). The positioning quality was better in group B, with 70% of patients achieving an optimal position compared to only 10% in group F ( P = 0.02).
Conclusions: Ultrasound-guided SFICB, as compared to systemic fentanyl, provided better analgesia and helped to achieve a better and more comfortable position to perform the neuraxial block.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


