Emma Kroeze, Dilys D. Weijers, Michelle M. Kleisman, Uri Ilan, Reno S. Bladergroen, Rico Hagelaar, Jules P. P. Meijerink, Marjolijn C. J. Jongmans, Jan L. C. Loeffen, Roland P. Kuiper
{"title":"T-cell lymphoblastic lymphoma in constitutional mismatch repair deficiency (CMMRD): Exploring treatment opportunities","authors":"Emma Kroeze, Dilys D. Weijers, Michelle M. Kleisman, Uri Ilan, Reno S. Bladergroen, Rico Hagelaar, Jules P. P. Meijerink, Marjolijn C. J. Jongmans, Jan L. C. Loeffen, Roland P. Kuiper","doi":"10.1002/hem3.73","DOIUrl":null,"url":null,"abstract":"<p>Constitutional mismatch repair deficiency (CMMRD) is a high-risk childhood cancer predisposition syndrome caused by biallelic germline mutations in one of the four mismatch repair (MMR) genes <i>MLH1</i>, <i>MSH2</i>, <i>MSH6</i>, or <i>PMS2</i>. Defective MMR results in the rapid accumulation of mutations and the continuous development of malignancies from an early age. The tumor spectrum of CMMRD patients consists mostly of high-grade brain tumors, gastrointestinal (GI) tumors, and hematologic malignancies.<span><sup>1</sup></span> Hematologic malignancies in CMMRD patients are predominantly lymphomas, most of which are T-cell lymphoblastic lymphomas (T-LBLs).<span><sup>2, 3</sup></span> T-LBL is a malignancy of immature T cells, characterized by infiltration of blasts in the mediastinum and lymph nodes, with fewer than 25% blasts in the bone marrow.<span><sup>4, 5</sup></span> Treatment of T-LBL generally consists of 2-year multiagent chemotherapy (LBL2018, NCT04043494).</p><p>Intensive surveillance protocols for CMMRD patients allow for early detection of brain tumors and GI tumors, providing additional treatment options besides chemotherapy, such as radical surgical resection or radiotherapy.<span><sup>3</sup></span> Moreover, hypermutated brain and GI tumors have shown a good response to PD-1 inhibitors, with hypermutated being defined as >10 mutations/Mb (mut/Mb).<span><sup>6, 7</sup></span> Clinically relevant surveillance strategies for hematologic malignancies are not yet available and it has yet to be studied whether T-LBLs are hypermutated, like brain and GI tumors, and could therefore benefit from checkpoint inhibitors, such as PD-1 inhibitors, as well. Consequently, CMMRD-associated T-LBL is currently treated according to the standard of care treatment strategies for sporadic T-LBL. There are several reasons why standard-of-care treatment strategies might be suboptimal in CMMRD T-LBL patients. Since CMMRD T-LBL patients are often heavily pretreated for previous malignancies, they may have developed chemoresistance. Additionally, previous doses of intensive therapy make patients also more vulnerable to severe complications. Moreover, the current LBL chemotherapeutic backbone consists of a number of mutagenic agents that can cause additional mutations and contribute to the development of new malignancies in these patients.<span><sup>2</sup></span> Additionally, there are indications that MMR deficiency leads to inherent resistance to thiopurines,<span><sup>8-10</sup></span> an important component of T-LBL treatment strategies (LBL2018, NCT04043494). It could therefore be beneficial for CMMRD patients to adapt the LBL backbone by removing the partially toxic and ineffective chemotherapeutic agents and replacing them with other, more effective agents. Molecular characterization of CMMRD-associated T-LBL and sporadic T-LBL could provide insights into molecular similarities and differences between these malignancies, potentially resulting in alternative treatment options for CMMRD-associated T-LBL.<span><sup>3</sup></span></p><p>We included data from eight CMMRD patients, who developed a total of nine T-LBLs (CMMRD-associated T-LBL) and 38 sporadic T-LBL patients.<span><sup>11, 12</sup></span> The median age of the sporadic T-LBL patients was 10 years and the disease affected more males (<i>n</i> = 22) than females (<i>n</i> = 16) (58% males). Age and sex distribution were similar for CMMRD-associated T-LBL, with a median age of 10 years and 63% males. We performed whole-exome sequencing on tumor-normal pairs for all sporadic T-LBLs and seven CMMRD-associated T-LBLs, and whole-genome sequencing of tumor-normal pairs for two CMMRD-associated T-LBLs. Data processing was performed as described previously.<span><sup>11, 12</sup></span> Tumor mutational burden (TMB) was calculated from the filtered data<span><sup>11</sup></span> using only mutations that were located in coding regions, revealing a large difference between CMMRD-associated and sporadic T-LBL (mean 24.62 and 0.49 mut/Mb; <i>p</i> < 0.0001, Wilcoxon's rank-sum test). When comparing the TMB of single-nucleotide variants (SNVs) and small insertions and deletions (indels) separately, we also found a substantially higher TMB in CMMRD-associated T-LBL compared to sporadic T-LBL (<i>p</i> < 0.0001, Wilcoxon's rank-sum test) (Figure 1A,B). In total, five of the CMMRD-associated T-LBLs could be defined as hypermutated (range: 11.7–129 mut/Mb). Although the remaining four were not hypermutated by definition, the TMB of the latter was still substantially higher (range: 4–6.1 mut/Mb) compared to sporadic T-LBLs (median: 0.47 mut/Mb; range: 0.05–1.23 mut/Mb). Recent studies on brain tumors and GI-tract tumors have shown that a high number of indels in microsatellites in hypermutated tumors of CMMRD patients is associated with a good response to PD1 inhibitors, a class of checkpoint inhibitors.<span><sup>6</sup></span> In this study, we show that most CMMRD-associated T-LBLs could be defined as hypermutated and that all CMMRD-associated T-LBLs have a significantly higher mutational burden than sporadic T-LBLs, which is a promising indication that CMMRD-associated T-LBL could be a good candidate for PD1 inhibition. These checkpoint inhibitors might be an effective replacement of mutagenic agents or ineffective chemotherapeutic treatments such as thiopurines. Further studies are required to decide whether checkpoint inhibitors are effective and how they can be safely incorporated in the treatment of CMMRD-associated T-LBL.</p><p>Additionally, we investigated a personalized medicine approach for which we analyzed the coding mutations identified in the individual tumors to find additional targets in high-risk patients. We focused on SNVs and indels, as this is where CMMRD-associated T-LBLs have the largest genomic heterogeneity. The analysis revealed that in CMMRD-associated T-LBL, there was a minimum of one targetable event per tumor, with a range of 1–14 such events. These events could be targeted with available compounds or compounds under investigation in ongoing clinical trials (Supporting Information S1: Table 1). The most frequently detected targetable events included <i>NOTCH1</i>, <i>PIK3CD</i>, <i>SMARCA4</i>, and <i>BRCA2</i> mutations. In contrast, among sporadic T-LBL patients, only five out of 38 patients exhibited an event that can be targeted by either an existing compound or a currently active clinical trial. These data show that a personalized medicine approach could be of benefit for CMMRD-associated T-LBL and may result in alternative treatment options to supplement, or partially replace multiagent chemotherapy.</p><p>Lastly, we explored the frequency of aberrations known to drive sporadic T-LBL in CMMRD-associated T-LBL to study possible differences in the mechanism of development. Copy number aberrations (CNAs) were called by implementing GATK v4.0.1.2 best practices.<span><sup>13</sup></span> Genes located around the breakpoints were determined using the GenomicRanges package in R v3.6.1. CNAs larger than 20 Mb were included and visually validated using denoized models. Copy number deletions in <i>CDKN2A/B</i> locus on 9p21, which are frequently smaller than 20 Mb, were also included. The overall number of CNAs (>20 Mb or loss of 9p21) was significantly lower in CMMRD T-LBL compared to sporadic T-LBL (<i>p</i> = 0.0012; Wilcoxon's rank-sum test), in line with what has been previously described for brain tumors in CMMRD patients<span><sup>14</sup></span> (Figure 1C). The loss of tumor suppressor locus <i>CDKN2A/B</i> caused by (partial) loss of 9p21, which is the most frequently detected aberration in T-LBL, was not present in CMMRD-associated T-LBL (Supporting Information S1: Figure 1). A possible explanation for a lower number of CNAs in CMMRD T-LBL could be that these tumors acquire high numbers of SNVs and indels and might therefore not require additional CNAs for their survival and proliferation. Mutations in most other genes known to be involved in sporadic T-LBL could be detected in CMMRD-associated T-LBL as well (Figure 1D).</p><p>There is an urgent need to use alternative treatment options for CMMRD-associated T-LBL as the current backbone of LBL treatment contains multiple agents that are probably ineffective due to resistance mechanisms, or even harmful due to the introduction of mutations that possibly contribute to the development of second primary malignancies in CMMRD patients. In a molecular characterization comparing CMMRD-associated T-LBL to sporadic T-LBL, we found various potential alternative treatment options for CMMRD-associated T-LBL, including the possibility to use checkpoint inhibitors, as well as utilizing targetable events detected through a personalized medicine approach. Exploiting other treatment options could help to diminish the cumulative dose of, possibly ineffective and toxic, chemotherapy in these often heavily pretreated individuals, which may help to improve their life expectancy.</p><p>Emma Kroeze and Dilys D. Weijers performed the study and wrote the paper, Michelle M. Kleisman, Uri Ilan and Rico Hagelaar performed the data analysis, Reno S. Bladergroen performed the sequencing, Marjolijn C. J. Jongmans contributed data, Jules P. P. Meijerink received the funding, Jan L. C. Loeffen and Roland P. Kuiper supervised and designed the study. All authors read and approved the manuscript.</p><p>The authors declare no conflict of interest.</p><p>This study was sponsored by Kinderen Kankervrij Grant KiKa-393 (EK) and the Dutch Cancer Society grant KWF-12909 (DDW).</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 5","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.73","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.73","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Constitutional mismatch repair deficiency (CMMRD) is a high-risk childhood cancer predisposition syndrome caused by biallelic germline mutations in one of the four mismatch repair (MMR) genes MLH1, MSH2, MSH6, or PMS2. Defective MMR results in the rapid accumulation of mutations and the continuous development of malignancies from an early age. The tumor spectrum of CMMRD patients consists mostly of high-grade brain tumors, gastrointestinal (GI) tumors, and hematologic malignancies.1 Hematologic malignancies in CMMRD patients are predominantly lymphomas, most of which are T-cell lymphoblastic lymphomas (T-LBLs).2, 3 T-LBL is a malignancy of immature T cells, characterized by infiltration of blasts in the mediastinum and lymph nodes, with fewer than 25% blasts in the bone marrow.4, 5 Treatment of T-LBL generally consists of 2-year multiagent chemotherapy (LBL2018, NCT04043494).
Intensive surveillance protocols for CMMRD patients allow for early detection of brain tumors and GI tumors, providing additional treatment options besides chemotherapy, such as radical surgical resection or radiotherapy.3 Moreover, hypermutated brain and GI tumors have shown a good response to PD-1 inhibitors, with hypermutated being defined as >10 mutations/Mb (mut/Mb).6, 7 Clinically relevant surveillance strategies for hematologic malignancies are not yet available and it has yet to be studied whether T-LBLs are hypermutated, like brain and GI tumors, and could therefore benefit from checkpoint inhibitors, such as PD-1 inhibitors, as well. Consequently, CMMRD-associated T-LBL is currently treated according to the standard of care treatment strategies for sporadic T-LBL. There are several reasons why standard-of-care treatment strategies might be suboptimal in CMMRD T-LBL patients. Since CMMRD T-LBL patients are often heavily pretreated for previous malignancies, they may have developed chemoresistance. Additionally, previous doses of intensive therapy make patients also more vulnerable to severe complications. Moreover, the current LBL chemotherapeutic backbone consists of a number of mutagenic agents that can cause additional mutations and contribute to the development of new malignancies in these patients.2 Additionally, there are indications that MMR deficiency leads to inherent resistance to thiopurines,8-10 an important component of T-LBL treatment strategies (LBL2018, NCT04043494). It could therefore be beneficial for CMMRD patients to adapt the LBL backbone by removing the partially toxic and ineffective chemotherapeutic agents and replacing them with other, more effective agents. Molecular characterization of CMMRD-associated T-LBL and sporadic T-LBL could provide insights into molecular similarities and differences between these malignancies, potentially resulting in alternative treatment options for CMMRD-associated T-LBL.3
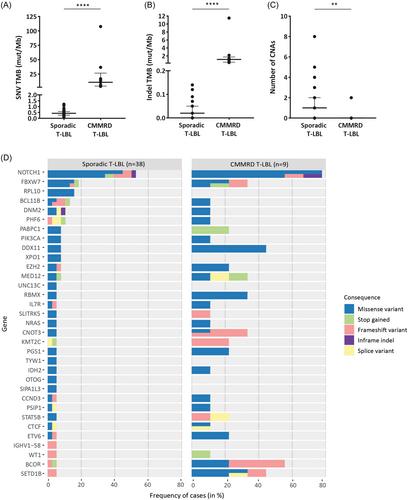
We included data from eight CMMRD patients, who developed a total of nine T-LBLs (CMMRD-associated T-LBL) and 38 sporadic T-LBL patients.11, 12 The median age of the sporadic T-LBL patients was 10 years and the disease affected more males (n = 22) than females (n = 16) (58% males). Age and sex distribution were similar for CMMRD-associated T-LBL, with a median age of 10 years and 63% males. We performed whole-exome sequencing on tumor-normal pairs for all sporadic T-LBLs and seven CMMRD-associated T-LBLs, and whole-genome sequencing of tumor-normal pairs for two CMMRD-associated T-LBLs. Data processing was performed as described previously.11, 12 Tumor mutational burden (TMB) was calculated from the filtered data11 using only mutations that were located in coding regions, revealing a large difference between CMMRD-associated and sporadic T-LBL (mean 24.62 and 0.49 mut/Mb; p < 0.0001, Wilcoxon's rank-sum test). When comparing the TMB of single-nucleotide variants (SNVs) and small insertions and deletions (indels) separately, we also found a substantially higher TMB in CMMRD-associated T-LBL compared to sporadic T-LBL (p < 0.0001, Wilcoxon's rank-sum test) (Figure 1A,B). In total, five of the CMMRD-associated T-LBLs could be defined as hypermutated (range: 11.7–129 mut/Mb). Although the remaining four were not hypermutated by definition, the TMB of the latter was still substantially higher (range: 4–6.1 mut/Mb) compared to sporadic T-LBLs (median: 0.47 mut/Mb; range: 0.05–1.23 mut/Mb). Recent studies on brain tumors and GI-tract tumors have shown that a high number of indels in microsatellites in hypermutated tumors of CMMRD patients is associated with a good response to PD1 inhibitors, a class of checkpoint inhibitors.6 In this study, we show that most CMMRD-associated T-LBLs could be defined as hypermutated and that all CMMRD-associated T-LBLs have a significantly higher mutational burden than sporadic T-LBLs, which is a promising indication that CMMRD-associated T-LBL could be a good candidate for PD1 inhibition. These checkpoint inhibitors might be an effective replacement of mutagenic agents or ineffective chemotherapeutic treatments such as thiopurines. Further studies are required to decide whether checkpoint inhibitors are effective and how they can be safely incorporated in the treatment of CMMRD-associated T-LBL.
Additionally, we investigated a personalized medicine approach for which we analyzed the coding mutations identified in the individual tumors to find additional targets in high-risk patients. We focused on SNVs and indels, as this is where CMMRD-associated T-LBLs have the largest genomic heterogeneity. The analysis revealed that in CMMRD-associated T-LBL, there was a minimum of one targetable event per tumor, with a range of 1–14 such events. These events could be targeted with available compounds or compounds under investigation in ongoing clinical trials (Supporting Information S1: Table 1). The most frequently detected targetable events included NOTCH1, PIK3CD, SMARCA4, and BRCA2 mutations. In contrast, among sporadic T-LBL patients, only five out of 38 patients exhibited an event that can be targeted by either an existing compound or a currently active clinical trial. These data show that a personalized medicine approach could be of benefit for CMMRD-associated T-LBL and may result in alternative treatment options to supplement, or partially replace multiagent chemotherapy.
Lastly, we explored the frequency of aberrations known to drive sporadic T-LBL in CMMRD-associated T-LBL to study possible differences in the mechanism of development. Copy number aberrations (CNAs) were called by implementing GATK v4.0.1.2 best practices.13 Genes located around the breakpoints were determined using the GenomicRanges package in R v3.6.1. CNAs larger than 20 Mb were included and visually validated using denoized models. Copy number deletions in CDKN2A/B locus on 9p21, which are frequently smaller than 20 Mb, were also included. The overall number of CNAs (>20 Mb or loss of 9p21) was significantly lower in CMMRD T-LBL compared to sporadic T-LBL (p = 0.0012; Wilcoxon's rank-sum test), in line with what has been previously described for brain tumors in CMMRD patients14 (Figure 1C). The loss of tumor suppressor locus CDKN2A/B caused by (partial) loss of 9p21, which is the most frequently detected aberration in T-LBL, was not present in CMMRD-associated T-LBL (Supporting Information S1: Figure 1). A possible explanation for a lower number of CNAs in CMMRD T-LBL could be that these tumors acquire high numbers of SNVs and indels and might therefore not require additional CNAs for their survival and proliferation. Mutations in most other genes known to be involved in sporadic T-LBL could be detected in CMMRD-associated T-LBL as well (Figure 1D).
There is an urgent need to use alternative treatment options for CMMRD-associated T-LBL as the current backbone of LBL treatment contains multiple agents that are probably ineffective due to resistance mechanisms, or even harmful due to the introduction of mutations that possibly contribute to the development of second primary malignancies in CMMRD patients. In a molecular characterization comparing CMMRD-associated T-LBL to sporadic T-LBL, we found various potential alternative treatment options for CMMRD-associated T-LBL, including the possibility to use checkpoint inhibitors, as well as utilizing targetable events detected through a personalized medicine approach. Exploiting other treatment options could help to diminish the cumulative dose of, possibly ineffective and toxic, chemotherapy in these often heavily pretreated individuals, which may help to improve their life expectancy.
Emma Kroeze and Dilys D. Weijers performed the study and wrote the paper, Michelle M. Kleisman, Uri Ilan and Rico Hagelaar performed the data analysis, Reno S. Bladergroen performed the sequencing, Marjolijn C. J. Jongmans contributed data, Jules P. P. Meijerink received the funding, Jan L. C. Loeffen and Roland P. Kuiper supervised and designed the study. All authors read and approved the manuscript.
The authors declare no conflict of interest.
This study was sponsored by Kinderen Kankervrij Grant KiKa-393 (EK) and the Dutch Cancer Society grant KWF-12909 (DDW).
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


