Cetuximab plus FOLFOXIRI versus cetuximab plus FOLFOX as conversion regimen in RAS/BRAF wild-type patients with initially unresectable colorectal liver metastases (TRICE trial): A randomized controlled trial.
{"title":"Cetuximab plus FOLFOXIRI versus cetuximab plus FOLFOX as conversion regimen in RAS/BRAF wild-type patients with initially unresectable colorectal liver metastases (TRICE trial): A randomized controlled trial.","authors":"De-Shen Wang, Chao Ren, Shan-Shan Li, William Pat Fong, Xiao-Jun Wu, Jian Xiao, Bin-Kui Li, Yun Zheng, Pei-Rong Ding, Gong Chen, Miao-Zhen Qiu, Zhi-Qiang Wang, Feng-Hua Wang, Hui-Yan Luo, Feng Wang, Xiao-Zhong Wang, Ling-Yun Wang, De-Jin Xie, Tao Chen, Li-Ren Li, Zhen-Hai Lu, Xiao-Hui Zhai, Tian-Shu Liu, Ying Yuan, Jia-Qi Chen, Qiong Tan, Zhi-Zhong Pan, De-Sen Wan, Rong Zhang, Yun-Fei Yuan, Rui-Hua Xu, Yu-Hong Li","doi":"10.1371/journal.pmed.1004389","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It remains unclear whether intensification of the chemotherapy backbone in tandem with an anti-EGFR can confer superior clinical outcomes in a cohort of RAS/BRAF wild-type colorectal cancer (CRC) patients with initially unresectable colorectal liver metastases (CRLM). To that end, we sought to comparatively evaluate the efficacy and safety of cetuximab plus FOLFOXIRI (triplet arm) versus cetuximab plus FOLFOX (doublet arm) as a conversion regimen (i.e., unresectable to resectable) in CRC patients with unresectable CRLM.</p><p><strong>Methods and findings: </strong>This open-label, randomized clinical trial was conducted from April 2018 to December 2022 in 7 medical centers across China, enrolling 146 RAS/BRAF wild-type CRC patients with initially unresectable CRLM. A stratified blocked randomization method was utilized to assign patients (1:1) to either the cetuximab plus FOLFOXIRI (n = 72) or cetuximab plus FOLFOX (n = 74) treatment arms. Stratification factors were tumor location (left versus right) and resectability (technically unresectable versus ≥5 metastases). The primary outcome was the objective response rate (ORR). Secondary outcomes included the median depth of tumor response (DpR), early tumor shrinkage (ETS), R0 resection rate, progression-free survival (PFS), overall survival (not mature at the time of analysis), and safety profile. Radiological tumor evaluations were conducted by radiologists blinded to the group allocation. Primary efficacy analyses were conducted based on the intention-to-treat population, while safety analyses were performed on patients who received at least 1 line of chemotherapy. A total of 14 patients (9.6%) were lost to follow-up (9 in the doublet arm and 5 in the triplet arm). The ORR was comparable following adjustment for stratification factors, with 84.7% versus 79.7% in the triplet and doublet arms, respectively (odds ratio [OR] 0.70; 95% confidence intervals [CI] [0.30, 1.67], Chi-square p = 0.42). Moreover, the ETS rate showed no significant difference between the triplet and doublet arms (80.6% (58/72) versus 77.0% (57/74), OR 0.82, 95% CI [0.37, 1.83], Chi-square p = 0.63). Although median DpR was higher in the triplet therapy group (59.6%, interquartile range [IQR], [50.0, 69.7] versus 55.0%, IQR [42.8, 63.8], Mann-Whitney p = 0.039), the R0/R1 resection rate with or without radiofrequency ablation/stereotactic body radiation therapy was comparable with 54.2% (39/72) of patients in the triplet arm versus 52.7% (39/74) in the doublet arm. At a median follow-up of 26.2 months (IQR [12.8, 40.5]), the median PFS was 11.8 months in the triplet arm versus 13.4 months in the doublet arm (hazard ratio [HR] 0.74, 95% CI [0.50, 1.11], Log-rank p = 0.14). Grade ≥ 3 events were reported in 47.2% (35/74) of patients in the doublet arm and 55.9% (38/68) of patients in the triplet arm. The triplet arm was associated with a higher incidence of grade ≥ 3 neutropenia (44.1% versus 27.0%, p = 0.03) and diarrhea (5.9% versus 0%, p = 0.03). The primary limitations of the study encompass the inherent bias in subjective surgical decisions regarding resection feasibility, as well as the lack of a centralized assessment for ORR and resection.</p><p><strong>Conclusions: </strong>The combination of cetuximab with FOLFOXIRI did not significantly improve ORR compared to cetuximab plus FOLFOX. Despite achieving an enhanced DpR, this improvement did not translate into improved R0 resection rates or PFS. Moreover, the triplet arm was associated with an increase in treatment-related toxicity.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT03493048.</p>","PeriodicalId":49008,"journal":{"name":"PLoS Medicine","volume":"21 5","pages":"e1004389"},"PeriodicalIF":9.9000,"publicationDate":"2024-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11086847/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1004389","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: It remains unclear whether intensification of the chemotherapy backbone in tandem with an anti-EGFR can confer superior clinical outcomes in a cohort of RAS/BRAF wild-type colorectal cancer (CRC) patients with initially unresectable colorectal liver metastases (CRLM). To that end, we sought to comparatively evaluate the efficacy and safety of cetuximab plus FOLFOXIRI (triplet arm) versus cetuximab plus FOLFOX (doublet arm) as a conversion regimen (i.e., unresectable to resectable) in CRC patients with unresectable CRLM.
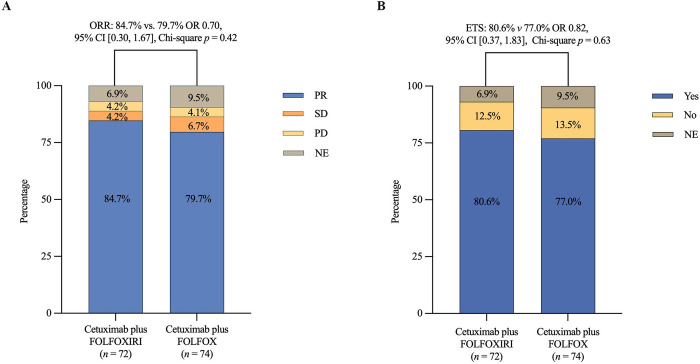
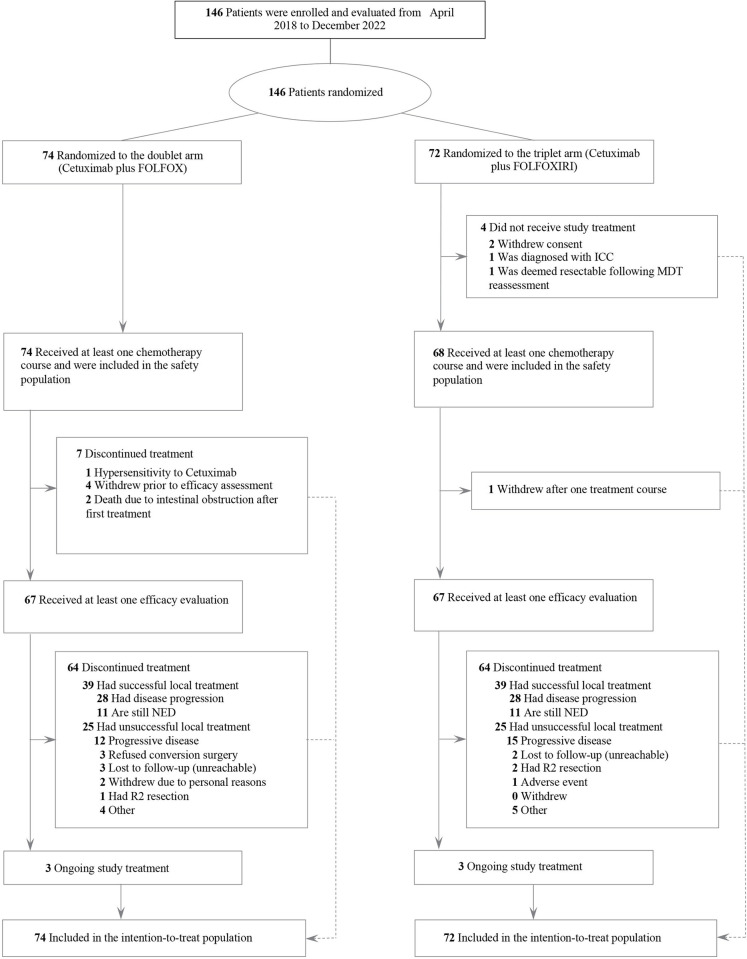
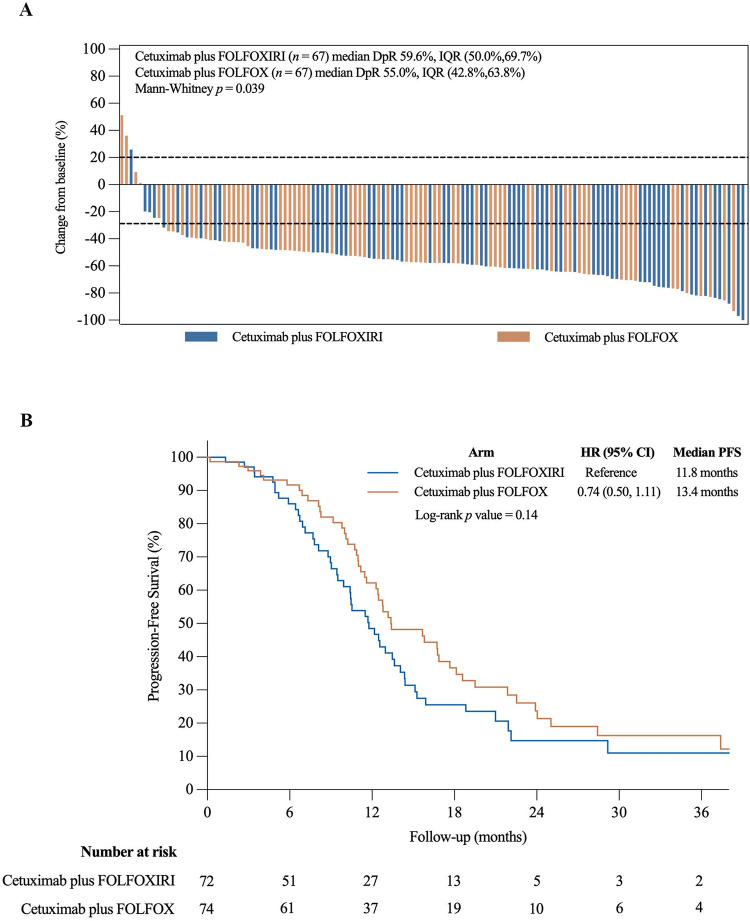
Methods and findings: This open-label, randomized clinical trial was conducted from April 2018 to December 2022 in 7 medical centers across China, enrolling 146 RAS/BRAF wild-type CRC patients with initially unresectable CRLM. A stratified blocked randomization method was utilized to assign patients (1:1) to either the cetuximab plus FOLFOXIRI (n = 72) or cetuximab plus FOLFOX (n = 74) treatment arms. Stratification factors were tumor location (left versus right) and resectability (technically unresectable versus ≥5 metastases). The primary outcome was the objective response rate (ORR). Secondary outcomes included the median depth of tumor response (DpR), early tumor shrinkage (ETS), R0 resection rate, progression-free survival (PFS), overall survival (not mature at the time of analysis), and safety profile. Radiological tumor evaluations were conducted by radiologists blinded to the group allocation. Primary efficacy analyses were conducted based on the intention-to-treat population, while safety analyses were performed on patients who received at least 1 line of chemotherapy. A total of 14 patients (9.6%) were lost to follow-up (9 in the doublet arm and 5 in the triplet arm). The ORR was comparable following adjustment for stratification factors, with 84.7% versus 79.7% in the triplet and doublet arms, respectively (odds ratio [OR] 0.70; 95% confidence intervals [CI] [0.30, 1.67], Chi-square p = 0.42). Moreover, the ETS rate showed no significant difference between the triplet and doublet arms (80.6% (58/72) versus 77.0% (57/74), OR 0.82, 95% CI [0.37, 1.83], Chi-square p = 0.63). Although median DpR was higher in the triplet therapy group (59.6%, interquartile range [IQR], [50.0, 69.7] versus 55.0%, IQR [42.8, 63.8], Mann-Whitney p = 0.039), the R0/R1 resection rate with or without radiofrequency ablation/stereotactic body radiation therapy was comparable with 54.2% (39/72) of patients in the triplet arm versus 52.7% (39/74) in the doublet arm. At a median follow-up of 26.2 months (IQR [12.8, 40.5]), the median PFS was 11.8 months in the triplet arm versus 13.4 months in the doublet arm (hazard ratio [HR] 0.74, 95% CI [0.50, 1.11], Log-rank p = 0.14). Grade ≥ 3 events were reported in 47.2% (35/74) of patients in the doublet arm and 55.9% (38/68) of patients in the triplet arm. The triplet arm was associated with a higher incidence of grade ≥ 3 neutropenia (44.1% versus 27.0%, p = 0.03) and diarrhea (5.9% versus 0%, p = 0.03). The primary limitations of the study encompass the inherent bias in subjective surgical decisions regarding resection feasibility, as well as the lack of a centralized assessment for ORR and resection.
Conclusions: The combination of cetuximab with FOLFOXIRI did not significantly improve ORR compared to cetuximab plus FOLFOX. Despite achieving an enhanced DpR, this improvement did not translate into improved R0 resection rates or PFS. Moreover, the triplet arm was associated with an increase in treatment-related toxicity.
期刊介绍:
PLOS Medicine is a prominent platform for discussing and researching global health challenges. The journal covers a wide range of topics, including biomedical, environmental, social, and political factors affecting health. It prioritizes articles that contribute to clinical practice, health policy, or a better understanding of pathophysiology, ultimately aiming to improve health outcomes across different settings.
The journal is unwavering in its commitment to uphold the highest ethical standards in medical publishing. This includes actively managing and disclosing any conflicts of interest related to reporting, reviewing, and publishing. PLOS Medicine promotes transparency in the entire review and publication process. The journal also encourages data sharing and encourages the reuse of published work. Additionally, authors retain copyright for their work, and the publication is made accessible through Open Access with no restrictions on availability and dissemination.
PLOS Medicine takes measures to avoid conflicts of interest associated with advertising drugs and medical devices or engaging in the exclusive sale of reprints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


