{"title":"Hyperventilation-induced cerebellar fit in a patient with Chiari 1.5 malformation","authors":"Ryota Sasaki, Masako Kinoshita, Nahomi Osugi, Hidehiro Hirabayashi, Ichiro Nakagawa","doi":"10.1002/epd2.20236","DOIUrl":null,"url":null,"abstract":"<p>Cerebellar fit (CF) is characterized by paroxysmal head retroflexion and opisthotonus with preserved consciousness.<span><sup>1-3</sup></span> Here, we present a case of a 43-year-old male with cough syncope (CS) due to Chiari 1.5 malformation, who exhibited CF during hyperventilation (HV).<span><sup>4</sup></span> EEG revealed a normal posterior dominant rhythm of 8–9 Hz. Approximately 150 s after initiating HV, the patient experienced truncal convulsion accompanied by opisthotonic posturing (Video 1). Notably, the patient retained his consciousness with open eyes. No electrographic seizure patterns were evident, the posterior dominant rhythm was preserved, and the electrocardiogram demonstrated normal sinus rhythm (Figure 1). He underwent a foramen magnum decompression and his CS and CF disappeared. As a mechanism, HV may induce dissociation between intracranial and spinal cord cerebrospinal fluid pressures, which further lower the cerebellum and compress the brainstem and cerebellum.<span><sup>2-5</sup></span> CF may be caused by the Guillain–Mollaret triangle disruption and CS by dysfunction of the brainstem reticular formation.<span><sup>6, 7</sup></span></p><p>This study was partially supported by JPJSBP 120217720 and by the Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering : Technology Exchange Program.</p><p>None of the authors have any conflicts of interest to declare.</p>","PeriodicalId":50508,"journal":{"name":"Epileptic Disorders","volume":"26 4","pages":"556-558"},"PeriodicalIF":1.9000,"publicationDate":"2024-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20236","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epileptic Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20236","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
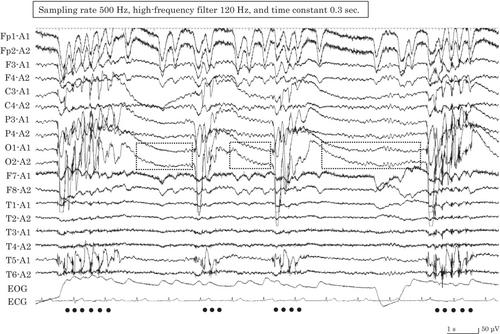
Cerebellar fit (CF) is characterized by paroxysmal head retroflexion and opisthotonus with preserved consciousness.1-3 Here, we present a case of a 43-year-old male with cough syncope (CS) due to Chiari 1.5 malformation, who exhibited CF during hyperventilation (HV).4 EEG revealed a normal posterior dominant rhythm of 8–9 Hz. Approximately 150 s after initiating HV, the patient experienced truncal convulsion accompanied by opisthotonic posturing (Video 1). Notably, the patient retained his consciousness with open eyes. No electrographic seizure patterns were evident, the posterior dominant rhythm was preserved, and the electrocardiogram demonstrated normal sinus rhythm (Figure 1). He underwent a foramen magnum decompression and his CS and CF disappeared. As a mechanism, HV may induce dissociation between intracranial and spinal cord cerebrospinal fluid pressures, which further lower the cerebellum and compress the brainstem and cerebellum.2-5 CF may be caused by the Guillain–Mollaret triangle disruption and CS by dysfunction of the brainstem reticular formation.6, 7
This study was partially supported by JPJSBP 120217720 and by the Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering : Technology Exchange Program.
None of the authors have any conflicts of interest to declare.
期刊介绍:
Epileptic Disorders is the leading forum where all experts and medical studentswho wish to improve their understanding of epilepsy and related disorders can share practical experiences surrounding diagnosis and care, natural history, and management of seizures.
Epileptic Disorders is the official E-journal of the International League Against Epilepsy for educational communication. As the journal celebrates its 20th anniversary, it will now be available only as an online version. Its mission is to create educational links between epileptologists and other health professionals in clinical practice and scientists or physicians in research-based institutions. This change is accompanied by an increase in the number of issues per year, from 4 to 6, to ensure regular diffusion of recently published material (high quality Review and Seminar in Epileptology papers; Original Research articles or Case reports of educational value; MultiMedia Teaching Material), to serve the global medical community that cares for those affected by epilepsy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


