Julie Marie Akers, Jennifer C Miller, Brandy Seignemartin, Linda Garrelts MacLean, Bidisha Mandal, Clark Kogan
{"title":"Expanding Access to Patient Care in Community Pharmacies for Minor Illnesses in Washington State.","authors":"Julie Marie Akers, Jennifer C Miller, Brandy Seignemartin, Linda Garrelts MacLean, Bidisha Mandal, Clark Kogan","doi":"10.2147/CEOR.S452743","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>As the shortage of primary care providers widens nationwide, access to care utilizing non-physician providers is one strategy to ensure equitable access to care. This study aimed to compare community pharmacist-provided care for minor ailments to care provided at three traditional sites of care: primary care, urgent care, and emergency department, to determine if care provided by pharmacists improved access with comparable quality and reduced financial strain on the healthcare system.</p><p><strong>Methods: </strong>Pharmacy data was provided from 46 pharmacies and 175 pharmacists who participated across five pharmacy corporations over a 3-year period (2016-2019). Data for non-pharmacy sites of care was provided by a large health plan, matching episodes of care for conditions seen in the community pharmacy. Cost-of-care analysis was conducted using superiority study design and revisit data analysis was conducted using noninferiority study design.</p><p><strong>Results: </strong>Median cost-of-care across traditional sites of care was $277.78 higher than care provided at the pharmacies, showing superiority. Noninferiority was demonstrated for revisit care when the initial visit was conducted by a pharmacist compared to traditional sites.</p><p><strong>Discussion: </strong>The authors conclude community pharmacist-provided care for minor ailments improved cost-effective access for patients with comparable quality and reduced financial strains on the healthcare system.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"16 ","pages":"233-246"},"PeriodicalIF":2.2000,"publicationDate":"2024-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11075675/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S452743","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: As the shortage of primary care providers widens nationwide, access to care utilizing non-physician providers is one strategy to ensure equitable access to care. This study aimed to compare community pharmacist-provided care for minor ailments to care provided at three traditional sites of care: primary care, urgent care, and emergency department, to determine if care provided by pharmacists improved access with comparable quality and reduced financial strain on the healthcare system.
Methods: Pharmacy data was provided from 46 pharmacies and 175 pharmacists who participated across five pharmacy corporations over a 3-year period (2016-2019). Data for non-pharmacy sites of care was provided by a large health plan, matching episodes of care for conditions seen in the community pharmacy. Cost-of-care analysis was conducted using superiority study design and revisit data analysis was conducted using noninferiority study design.
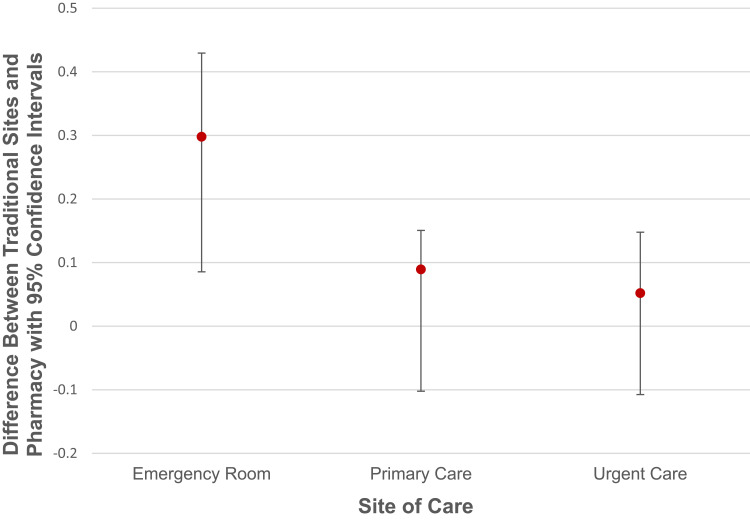
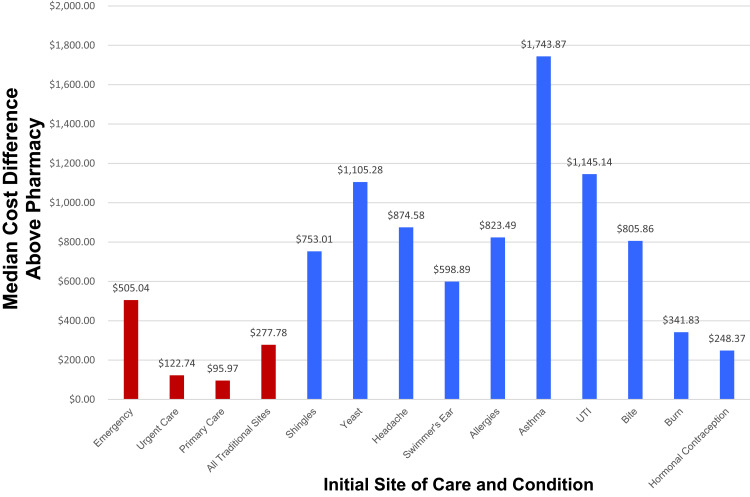
Results: Median cost-of-care across traditional sites of care was $277.78 higher than care provided at the pharmacies, showing superiority. Noninferiority was demonstrated for revisit care when the initial visit was conducted by a pharmacist compared to traditional sites.
Discussion: The authors conclude community pharmacist-provided care for minor ailments improved cost-effective access for patients with comparable quality and reduced financial strains on the healthcare system.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


