{"title":"Novel clip closure technique for a large mucosal defect with anchor-pronged clips after duodenal endoscopic submucosal dissection","authors":"Kohei Shigeta, Noboru Kawata, Hiroyuki Ono","doi":"10.1111/den.14813","DOIUrl":null,"url":null,"abstract":"<p>Duodenal endoscopic submucosal dissection (DESD) has a high incidence of delayed adverse events (AEs).<span><sup>1</sup></span> However, complete mucosal closure (CMC) can reduce the risk of AEs after DESD.<span><sup>2</sup></span> Conventional clip closure is a common technique,<span><sup>1</sup></span> but it poses challenges when used for CMC of large defects after DESD. This case shows a simple closure technique using anchor-pronged clips (MANTIS clip; Boston Scientific, Waltham, MA, USA) for CMC after DESD.</p><p>A 63-year-old man underwent DESD for a 40 mm flat elevated lesion in the descending duodenum (Fig. 1a). During the DESD, an intraprocedural perforation occurred, which was closed using a conventional clip (SureClip; Micro-tech, Nanjing, China). Then en bloc resection was performed on a 47 × 41 mm specimen (Fig. 1b). After resection, mucosal closure was initiated with the anchor-pronged clips for the approximately half circumferential defect (Fig. 2a,b). We grasped the oral edge of the defect using the anchor-pronged clip, allowing us to bring and grasp the opposite side (Video S1). The anchor-pronged clip closed the center of the defect (Fig. 2c), and CMC was achieved in 11 min using seven additional conventional clips (Fig. 2d). The patient was discharged 6 days later without AEs. Pathological examination revealed the lesion was an intramucosal well-differentiated adenocarcinoma with negative resection margins.</p><p>Although there are various techniques for CMC after DESD,<span><sup>1</sup></span> some of these methods require technical skills. Anchor-pronged clip closure is a simple technique that enables the closure of larger defects and overcomes the challenges of conventional clips during the closure procedure, such as tissue slippage when grasping the opposite side.<span><sup>3, 4</sup></span> Furthermore, by applying the previously reported technique of anchor-pronged clip to grasp and suture the muscle layer, it may be possible to reduce suture-induced dead space even in the duodenum.<span><sup>5</sup></span> Therefore, mucosal closure using anchor-pronged clips is a viable option for CMC of large defects after DESD.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 7","pages":"849-850"},"PeriodicalIF":5.0000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14813","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14813","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Duodenal endoscopic submucosal dissection (DESD) has a high incidence of delayed adverse events (AEs).1 However, complete mucosal closure (CMC) can reduce the risk of AEs after DESD.2 Conventional clip closure is a common technique,1 but it poses challenges when used for CMC of large defects after DESD. This case shows a simple closure technique using anchor-pronged clips (MANTIS clip; Boston Scientific, Waltham, MA, USA) for CMC after DESD.
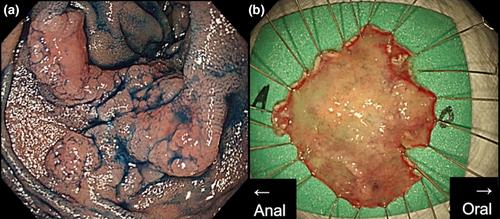
A 63-year-old man underwent DESD for a 40 mm flat elevated lesion in the descending duodenum (Fig. 1a). During the DESD, an intraprocedural perforation occurred, which was closed using a conventional clip (SureClip; Micro-tech, Nanjing, China). Then en bloc resection was performed on a 47 × 41 mm specimen (Fig. 1b). After resection, mucosal closure was initiated with the anchor-pronged clips for the approximately half circumferential defect (Fig. 2a,b). We grasped the oral edge of the defect using the anchor-pronged clip, allowing us to bring and grasp the opposite side (Video S1). The anchor-pronged clip closed the center of the defect (Fig. 2c), and CMC was achieved in 11 min using seven additional conventional clips (Fig. 2d). The patient was discharged 6 days later without AEs. Pathological examination revealed the lesion was an intramucosal well-differentiated adenocarcinoma with negative resection margins.
Although there are various techniques for CMC after DESD,1 some of these methods require technical skills. Anchor-pronged clip closure is a simple technique that enables the closure of larger defects and overcomes the challenges of conventional clips during the closure procedure, such as tissue slippage when grasping the opposite side.3, 4 Furthermore, by applying the previously reported technique of anchor-pronged clip to grasp and suture the muscle layer, it may be possible to reduce suture-induced dead space even in the duodenum.5 Therefore, mucosal closure using anchor-pronged clips is a viable option for CMC of large defects after DESD.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


