Federico Angriman, Jutamas Saoraya, Patrick R Lawler, Baiju R Shah, Claudio M Martin, Damon C Scales
{"title":"Preexisting Diabetes Mellitus and All-Cause Mortality in Adult Patients With Sepsis: A Population-Based Cohort Study.","authors":"Federico Angriman, Jutamas Saoraya, Patrick R Lawler, Baiju R Shah, Claudio M Martin, Damon C Scales","doi":"10.1097/CCE.0000000000001085","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We assessed the association of preexisting diabetes mellitus with all-cause mortality and organ support receipt in adult patients with sepsis.</p><p><strong>Design: </strong>Population-based cohort study.</p><p><strong>Setting: </strong>Ontario, Canada (2008-2019).</p><p><strong>Population: </strong>Adult patients (18 yr old or older) with a first sepsis-related hospitalization episode.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>The main exposure of interest was preexisting diabetes (either type 1 or 2). The primary outcome was all-cause mortality by 90 days; secondary outcomes included receipt of invasive mechanical ventilation and new renal replacement therapy. We report adjusted (for baseline characteristics using standardization) risk ratios (RRs) alongside 95% CIs. A main secondary analysis evaluated the potential mediation by prior metformin use of the association between preexisting diabetes and all-cause mortality following sepsis. Overall, 503,455 adults with a first sepsis-related hospitalization episode were included; 36% had preexisting diabetes. Mean age was 73 years, and 54% of the cohort were females. Preexisting diabetes was associated with a lower adjusted risk of all-cause mortality at 90 days (RR, 0.81; 95% CI, 0.80-0.82). Preexisting diabetes was associated with an increased risk of new renal replacement therapy (RR, 1.53; 95% CI, 1.46-1.60) but not invasive mechanical ventilation (RR, 1.03; 95% CI, 1.00-1.05). Overall, 21% (95% CI, 19-28) of the association between preexisting diabetes and reduced risk of all-cause mortality was mediated by prior metformin use.</p><p><strong>Conclusions: </strong>Preexisting diabetes is associated with a lower risk of all-cause mortality and higher risk of new renal replacement therapy among adult patients with sepsis. Future studies should evaluate the underlying mechanisms of these associations.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 5","pages":"e1085"},"PeriodicalIF":2.7000,"publicationDate":"2024-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11075944/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: We assessed the association of preexisting diabetes mellitus with all-cause mortality and organ support receipt in adult patients with sepsis.
Design: Population-based cohort study.
Setting: Ontario, Canada (2008-2019).
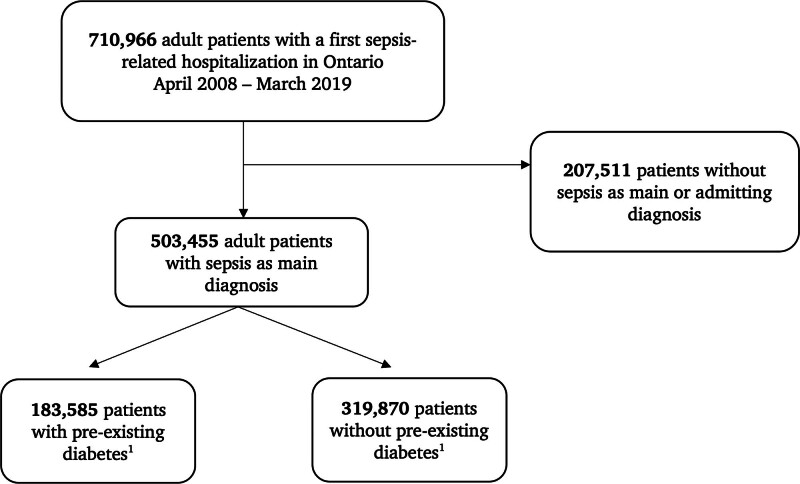
Population: Adult patients (18 yr old or older) with a first sepsis-related hospitalization episode.
Interventions: None.
Measurements and main results: The main exposure of interest was preexisting diabetes (either type 1 or 2). The primary outcome was all-cause mortality by 90 days; secondary outcomes included receipt of invasive mechanical ventilation and new renal replacement therapy. We report adjusted (for baseline characteristics using standardization) risk ratios (RRs) alongside 95% CIs. A main secondary analysis evaluated the potential mediation by prior metformin use of the association between preexisting diabetes and all-cause mortality following sepsis. Overall, 503,455 adults with a first sepsis-related hospitalization episode were included; 36% had preexisting diabetes. Mean age was 73 years, and 54% of the cohort were females. Preexisting diabetes was associated with a lower adjusted risk of all-cause mortality at 90 days (RR, 0.81; 95% CI, 0.80-0.82). Preexisting diabetes was associated with an increased risk of new renal replacement therapy (RR, 1.53; 95% CI, 1.46-1.60) but not invasive mechanical ventilation (RR, 1.03; 95% CI, 1.00-1.05). Overall, 21% (95% CI, 19-28) of the association between preexisting diabetes and reduced risk of all-cause mortality was mediated by prior metformin use.
Conclusions: Preexisting diabetes is associated with a lower risk of all-cause mortality and higher risk of new renal replacement therapy among adult patients with sepsis. Future studies should evaluate the underlying mechanisms of these associations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


