Katrine Fjaellegaard, Jesper Koefod Petersen, Gitte Alstrup, Søren Skaarup, Paul Frost Clementsen, Christian B Laursen, Rahul Bhatnagar, Uffe Bodtger
{"title":"Ultrasound in predicting improvement in dyspnoea after therapeutic thoracentesis in patients with recurrent unilateral pleural effusion.","authors":"Katrine Fjaellegaard, Jesper Koefod Petersen, Gitte Alstrup, Søren Skaarup, Paul Frost Clementsen, Christian B Laursen, Rahul Bhatnagar, Uffe Bodtger","doi":"10.1080/20018525.2024.2337446","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with recurrent pleural effusion, therapeutic thoracentesis is one way of relief. Correct prediction of which patients will experience relief following drainage may support the management of these patients. This study aimed to assess the association between ultrasound (US) characteristics and a relevant improvement in dyspnoea immediately following drainage.</p><p><strong>Methods: </strong>In a prospective, observational study, patients with recurrent unilateral pleural effusion underwent US evaluation of effusion characteristics and diaphragm movement measured by M-mode and the Area method before and right after drainage. The level of dyspnoea was assessed using the modified Borg scale (MBS). A minimal important improvement in dyspnoea was defined as delta MBS ≥ 1.</p><p><strong>Results: </strong>In the 104 patients included, 53% had a minimal important improvement in dyspnoea following thoracentesis. We found no association between US-characteristics, including diaphragm shape or movement (M-mode or the Area method), and a decrease in dyspnoea following drainage. Baseline MBS score ≥ 4 and a fully drained effusion were significant correlated with a minimal important improvement in dyspnoea (OR 3.86 (1.42-10.50), <i>p</i> = 0.01 and 2.86 (1.03-7.93), <i>p</i> = 0.04, respectively).</p><p><strong>Conclusions: </strong>In our study population, US-characteristics including assessment of diaphragm movement or shape was not associated with a minimal important improvement in dyspnoea immediately following thoracentesis.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"11 1","pages":"2337446"},"PeriodicalIF":1.4000,"publicationDate":"2024-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11073413/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2024.2337446","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with recurrent pleural effusion, therapeutic thoracentesis is one way of relief. Correct prediction of which patients will experience relief following drainage may support the management of these patients. This study aimed to assess the association between ultrasound (US) characteristics and a relevant improvement in dyspnoea immediately following drainage.
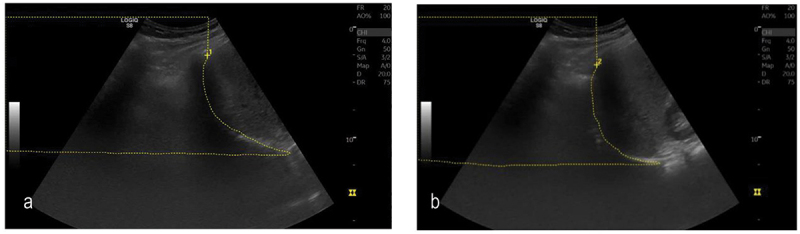
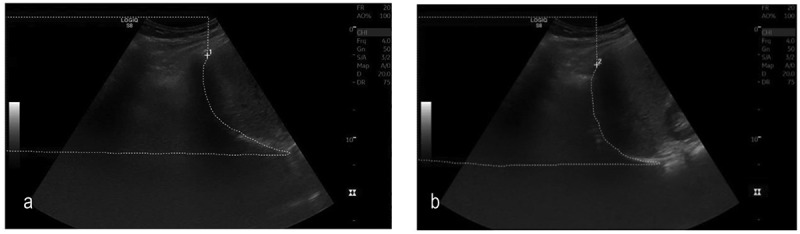
Methods: In a prospective, observational study, patients with recurrent unilateral pleural effusion underwent US evaluation of effusion characteristics and diaphragm movement measured by M-mode and the Area method before and right after drainage. The level of dyspnoea was assessed using the modified Borg scale (MBS). A minimal important improvement in dyspnoea was defined as delta MBS ≥ 1.
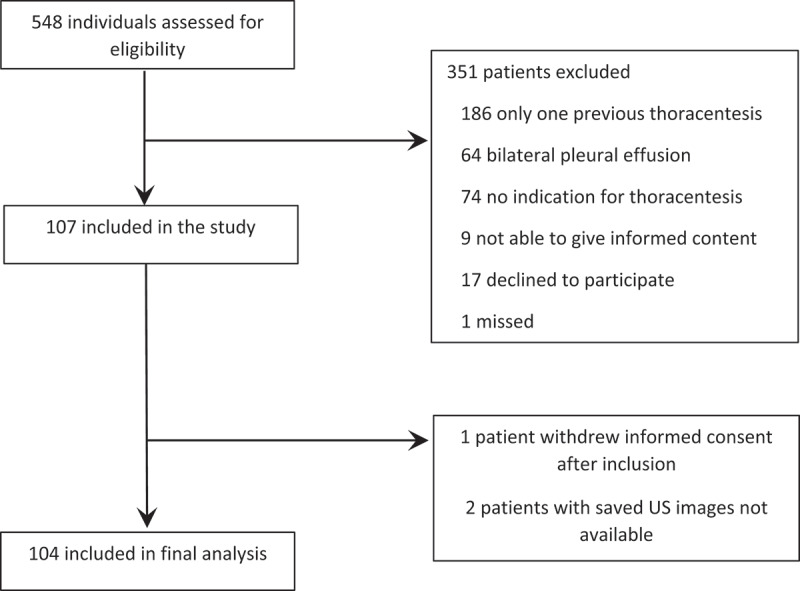
Results: In the 104 patients included, 53% had a minimal important improvement in dyspnoea following thoracentesis. We found no association between US-characteristics, including diaphragm shape or movement (M-mode or the Area method), and a decrease in dyspnoea following drainage. Baseline MBS score ≥ 4 and a fully drained effusion were significant correlated with a minimal important improvement in dyspnoea (OR 3.86 (1.42-10.50), p = 0.01 and 2.86 (1.03-7.93), p = 0.04, respectively).
Conclusions: In our study population, US-characteristics including assessment of diaphragm movement or shape was not associated with a minimal important improvement in dyspnoea immediately following thoracentesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


