Eunjin Park, Junghyeon Park, So-Youn Chang, Youngkook Kim
{"title":"Nontraumatic Myositis Ossificans After Spontaneous Subarachnoid Hemorrhage: A Case Report.","authors":"Eunjin Park, Junghyeon Park, So-Youn Chang, Youngkook Kim","doi":"10.12786/bn.2024.17.e9","DOIUrl":null,"url":null,"abstract":"<p><p>Myositis ossificans is uncommon in patients with nontraumatic brain injuries. This report presents a challenging case in which myositis ossificans was diagnosed and treated by medical management in a patient who was unable to complain of any symptoms due to akinetic mutism that occurred after nontraumatic subarachnoid hemorrhage. The patient had intermittent high-grade fever, and laboratory tests showed elevated C-reactive protein and D-dimer levels without clinical signs of infection two months after subarachnoid hemorrhage. Lower-extremity venography using computed tomography was performed to rule out deep venous thrombosis. There was no thrombus, but right vastus medialis muscle showed inflammatory change with faint multilayered curvilinear hyperdense rims. The administration of indomethacin helped prevent abnormal bone formation. For the early detection of myositis ossificans, careful observation of clinical presentation and a high index of clinical suspicion is necessary in brain-injured patients. Further, elevated serum inflammatory markers accompanied by elevated alkaline phosphatase can be a critical clue. Early computed tomography helps identify early 'string sign' prior to characteristic ossification. Our report highlights that the myositis ossificans is remediable by early detection and appropriate nonsurgical management.</p>","PeriodicalId":72442,"journal":{"name":"Brain & NeuroRehabilitation","volume":"17 1","pages":"e9"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10990839/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain & NeuroRehabilitation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12786/bn.2024.17.e9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
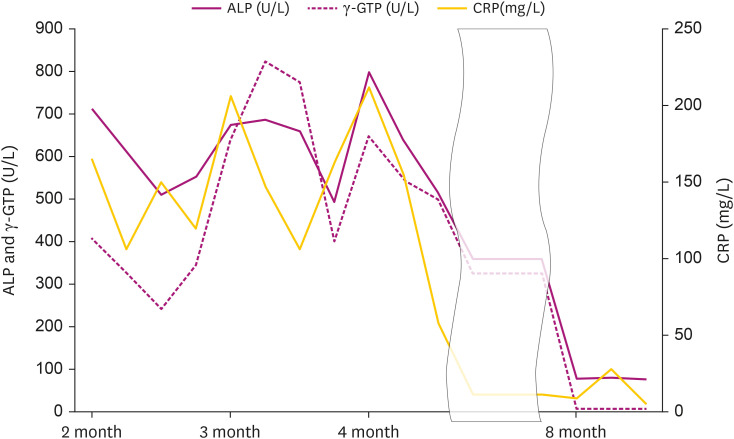
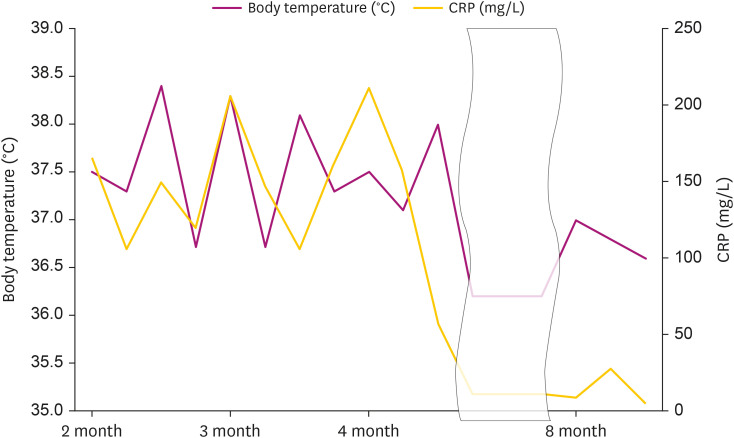
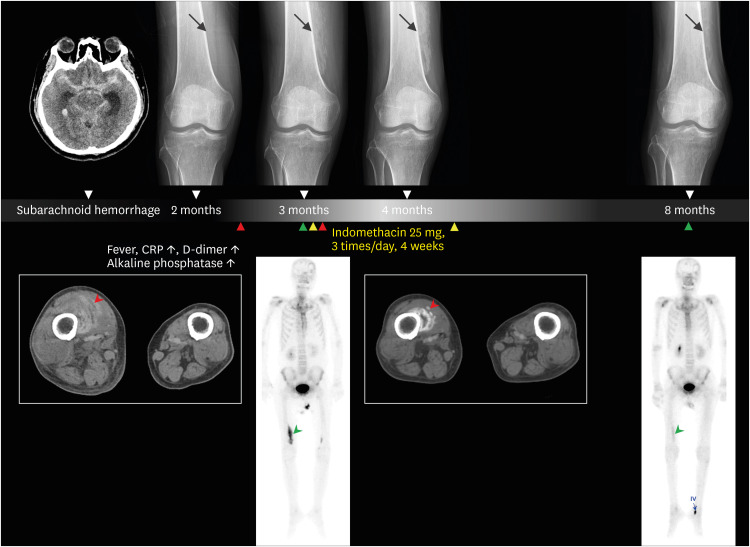
Myositis ossificans is uncommon in patients with nontraumatic brain injuries. This report presents a challenging case in which myositis ossificans was diagnosed and treated by medical management in a patient who was unable to complain of any symptoms due to akinetic mutism that occurred after nontraumatic subarachnoid hemorrhage. The patient had intermittent high-grade fever, and laboratory tests showed elevated C-reactive protein and D-dimer levels without clinical signs of infection two months after subarachnoid hemorrhage. Lower-extremity venography using computed tomography was performed to rule out deep venous thrombosis. There was no thrombus, but right vastus medialis muscle showed inflammatory change with faint multilayered curvilinear hyperdense rims. The administration of indomethacin helped prevent abnormal bone formation. For the early detection of myositis ossificans, careful observation of clinical presentation and a high index of clinical suspicion is necessary in brain-injured patients. Further, elevated serum inflammatory markers accompanied by elevated alkaline phosphatase can be a critical clue. Early computed tomography helps identify early 'string sign' prior to characteristic ossification. Our report highlights that the myositis ossificans is remediable by early detection and appropriate nonsurgical management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


