{"title":"Liver transplantation for hepatocellular carcinoma in India: Are we ready for 2040?","authors":"Hirak Pahari, Amruth Raj, Ambreen Sawant, Dipak S Ahire, Raosaheb Rathod, Chetan Rathi, Tushar Sankalecha, Sachin Palnitkar, Vikram Raut","doi":"10.5500/wjt.v14.i1.88833","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liver transplantation (LT) for hepatocellular carcinoma (HCC) has been widely researched and is well established worldwide. The cornerstone of this treatment lies in the various criteria formulated by expert consensus and experience. The variations among the criteria are staggering, and the short- and long-term out comes are controversial.</p><p><strong>Aim: </strong>To study the differences in the current practices of LT for HCC at different centers in India and discuss their clinical implications in the future.</p><p><strong>Methods: </strong>We conducted a survey of major centers in India that performed LT in December 2022. A total of 23 responses were received. The centers were classified as high- and low-volume, and the current trend of care for patients und ergoing LT for HCC was noted.</p><p><strong>Results: </strong>Of the 23 centers, 35% were high volume center (> 500 Liver transplants) while 52% were high-volume centers that performed more than 50 transplants/year. Approximately 39% of centers had performed > 50 LT for HCC while the percent distribution for HCC in LT patients was 5%-15% in approximately 73% of the patients. Barring a few, most centers were divided equally between University of California, San Francisco (UCSF) and center-specific criteria when choosing patients with HCC for LT, and most (65%) did not have separate transplant criteria for deceased donor LT and living donor LT (LDLT). Most centers (56%) preferred surgical resection over LT for a Child A cirrhosis patient with a resectable 4 cm HCC lesion. Positron-emission tomography-computed tomography (CT) was the modality of choice for metastatic workup in the majority of centers (74%). Downstaging was the preferred option for over 90% of the centers and included transarterial chemoembolization, transarterial radioembolization, stereotactic body radiotherapy and atezolizumab/bevacizumab with varied indications. The alpha-fetoprotein (AFP) cut-off was used by 74% of centers to decide on transplantation as well as to downstage tumors, even if they met the criteria. The criteria for successful downstaging varied, but most centers conformed to the UCSF or their center-specific criteria for LT, along with the AFP cutoff values. The wait time for LT from down staging was at least 4-6 wk in all centers. Contrast-enhanced CT was the preferred imaging modality for post-LT surveillance in 52% of the centers. Approximately 65% of the centers preferred to start everolimus between 1 and 3 months post-LT.</p><p><strong>Conclusion: </strong>The current predicted 5-year survival rate of HCC patients in India is less than 15%. The aim of transplantation is to achieve at least a 60% 5-year disease free survival rate, which will provide relief to the prediction of an HCC surge over the next 20 years. The current worldwide criteria (Milan/UCSF) may have a higher 5-year survival (> 70%); however, the majority of patients still do not fit these criteria and are dependent on other suboptimal modes of treatment, with much lower survival rates. To make predictions for 2040, we must prepare to arm ourselves with less stringent selection criteria to widen the pool of patients who may undergo transplantation and have a chance of a better outcome. With more advanced technology and better donor outcomes, LDLT will provide a cutting edge in the fight against liver cancer over the next two decades.</p>","PeriodicalId":68893,"journal":{"name":"世界移植杂志(英文版)","volume":"14 1","pages":"88833"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10989470/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5500/wjt.v14.i1.88833","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Liver transplantation (LT) for hepatocellular carcinoma (HCC) has been widely researched and is well established worldwide. The cornerstone of this treatment lies in the various criteria formulated by expert consensus and experience. The variations among the criteria are staggering, and the short- and long-term out comes are controversial.
Aim: To study the differences in the current practices of LT for HCC at different centers in India and discuss their clinical implications in the future.
Methods: We conducted a survey of major centers in India that performed LT in December 2022. A total of 23 responses were received. The centers were classified as high- and low-volume, and the current trend of care for patients und ergoing LT for HCC was noted.
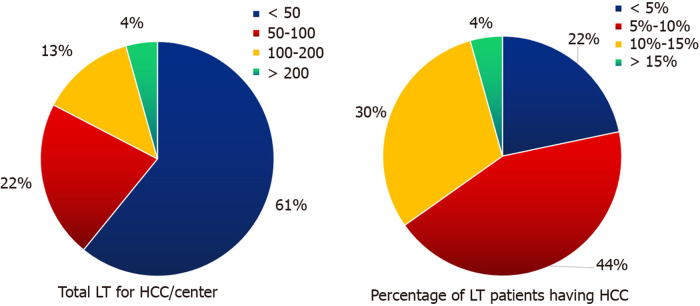
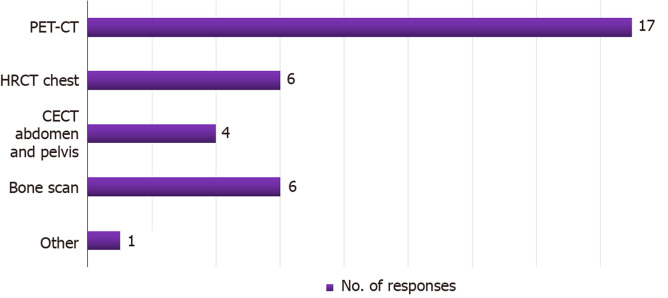
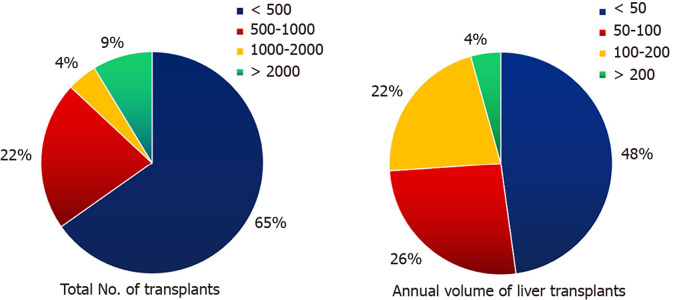
Results: Of the 23 centers, 35% were high volume center (> 500 Liver transplants) while 52% were high-volume centers that performed more than 50 transplants/year. Approximately 39% of centers had performed > 50 LT for HCC while the percent distribution for HCC in LT patients was 5%-15% in approximately 73% of the patients. Barring a few, most centers were divided equally between University of California, San Francisco (UCSF) and center-specific criteria when choosing patients with HCC for LT, and most (65%) did not have separate transplant criteria for deceased donor LT and living donor LT (LDLT). Most centers (56%) preferred surgical resection over LT for a Child A cirrhosis patient with a resectable 4 cm HCC lesion. Positron-emission tomography-computed tomography (CT) was the modality of choice for metastatic workup in the majority of centers (74%). Downstaging was the preferred option for over 90% of the centers and included transarterial chemoembolization, transarterial radioembolization, stereotactic body radiotherapy and atezolizumab/bevacizumab with varied indications. The alpha-fetoprotein (AFP) cut-off was used by 74% of centers to decide on transplantation as well as to downstage tumors, even if they met the criteria. The criteria for successful downstaging varied, but most centers conformed to the UCSF or their center-specific criteria for LT, along with the AFP cutoff values. The wait time for LT from down staging was at least 4-6 wk in all centers. Contrast-enhanced CT was the preferred imaging modality for post-LT surveillance in 52% of the centers. Approximately 65% of the centers preferred to start everolimus between 1 and 3 months post-LT.
Conclusion: The current predicted 5-year survival rate of HCC patients in India is less than 15%. The aim of transplantation is to achieve at least a 60% 5-year disease free survival rate, which will provide relief to the prediction of an HCC surge over the next 20 years. The current worldwide criteria (Milan/UCSF) may have a higher 5-year survival (> 70%); however, the majority of patients still do not fit these criteria and are dependent on other suboptimal modes of treatment, with much lower survival rates. To make predictions for 2040, we must prepare to arm ourselves with less stringent selection criteria to widen the pool of patients who may undergo transplantation and have a chance of a better outcome. With more advanced technology and better donor outcomes, LDLT will provide a cutting edge in the fight against liver cancer over the next two decades.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


