Alexander J Adamson, Constantinos Kallis, Ian Douglas, Jennifer K Quint
{"title":"Accuracy of the recording of pneumonia events in English electronic healthcare record data in patients with chronic obstructive pulmonary disease.","authors":"Alexander J Adamson, Constantinos Kallis, Ian Douglas, Jennifer K Quint","doi":"10.1186/s41479-024-00130-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In primary care, identifying pneumonia events in people with chronic obstructive pulmonary disease (COPD) may be challenging due to similarities in symptoms with COPD exacerbations and lack of diagnostic testing. This study explored the accuracy of pneumonia diagnosis coded in primary care by comparing diagnosis in primary care with diagnosis in hospital.</p><p><strong>Methods: </strong>A study population of people with COPD in England was created using the Clinical Practice Research Datalink Aurum database linked with Hospital Episode Statistics inpatient data. Pneumonia codes only, and pneumonia code with associated clinical and/or treatment codes (chest x-ray, symptoms, antibiotics, sputum and blood culture) were used to determine pneumonia events in primary care. Events that were followed by hospitalisation within 7 days were used to estimate the positive predictive value (PPV) of pneumonia coding in primary care, using primary diagnosis of pneumonia in secondary care as the gold standard. The PPV of primary care recording of hospitalised pneumonia was also calculated.</p><p><strong>Results: </strong>Two hundred seventy-four thousand one hundred fifty-six COPD patients were eligible for inclusion, of whom 7,560 had an eligible pneumonia event in primary care diagnosed between 2015-2019 which was not 'hospital-acquired' and was diagnosed and entered on the same day. Of the 2,094 events which were followed by hospitalisation within 7 days, 1,208 had a primary diagnosis of pneumonia in hospital, representing a PPV of pneumonia coding in primary care of 57.7% (95% CI 55.6%-59.8%). Another 284 (13.6%) were diagnosed as a COPD exacerbation and 114 (5.4%) were diagnosed as another respiratory disease. Use of additional pneumonia clinical and treatment codes had a modest effect on the PPV but substantially lowered the number of events. Of the 33,603 eligible pneumonia events identified in secondary care, only 11,445 were recorded in primary care within 42 days, representing a sensitivity of 34.1% (95% CI 33.6%-34.6%).</p><p><strong>Conclusions: </strong>Use of primary care pneumonia codes and associated clinical and treatment codes to determine pneumonia is not recommended due to significant levels of misdiagnosis and many hospitalised events failing to be recorded in primary care.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"16 1","pages":"8"},"PeriodicalIF":6.2000,"publicationDate":"2024-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11070075/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-024-00130-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In primary care, identifying pneumonia events in people with chronic obstructive pulmonary disease (COPD) may be challenging due to similarities in symptoms with COPD exacerbations and lack of diagnostic testing. This study explored the accuracy of pneumonia diagnosis coded in primary care by comparing diagnosis in primary care with diagnosis in hospital.
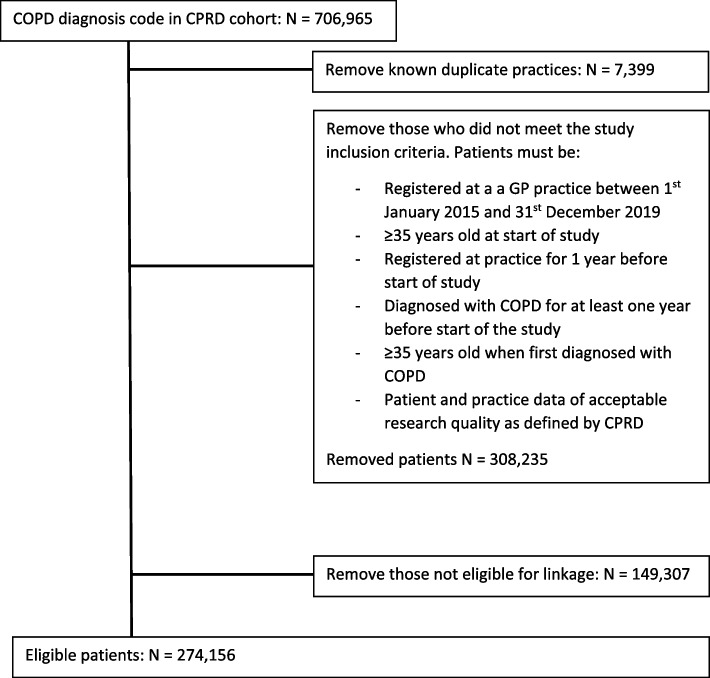
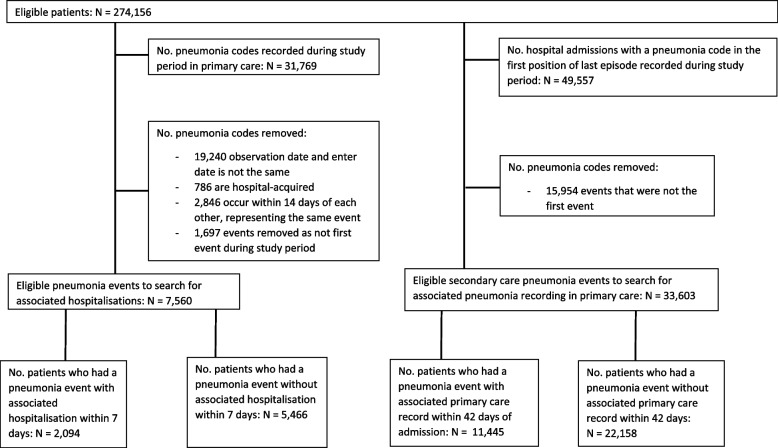
Methods: A study population of people with COPD in England was created using the Clinical Practice Research Datalink Aurum database linked with Hospital Episode Statistics inpatient data. Pneumonia codes only, and pneumonia code with associated clinical and/or treatment codes (chest x-ray, symptoms, antibiotics, sputum and blood culture) were used to determine pneumonia events in primary care. Events that were followed by hospitalisation within 7 days were used to estimate the positive predictive value (PPV) of pneumonia coding in primary care, using primary diagnosis of pneumonia in secondary care as the gold standard. The PPV of primary care recording of hospitalised pneumonia was also calculated.
Results: Two hundred seventy-four thousand one hundred fifty-six COPD patients were eligible for inclusion, of whom 7,560 had an eligible pneumonia event in primary care diagnosed between 2015-2019 which was not 'hospital-acquired' and was diagnosed and entered on the same day. Of the 2,094 events which were followed by hospitalisation within 7 days, 1,208 had a primary diagnosis of pneumonia in hospital, representing a PPV of pneumonia coding in primary care of 57.7% (95% CI 55.6%-59.8%). Another 284 (13.6%) were diagnosed as a COPD exacerbation and 114 (5.4%) were diagnosed as another respiratory disease. Use of additional pneumonia clinical and treatment codes had a modest effect on the PPV but substantially lowered the number of events. Of the 33,603 eligible pneumonia events identified in secondary care, only 11,445 were recorded in primary care within 42 days, representing a sensitivity of 34.1% (95% CI 33.6%-34.6%).
Conclusions: Use of primary care pneumonia codes and associated clinical and treatment codes to determine pneumonia is not recommended due to significant levels of misdiagnosis and many hospitalised events failing to be recorded in primary care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


