{"title":"Unusual rectal polyp","authors":"Chun-Chi Hsu, Yu-Chun Ma, Wen-Hung Hsu","doi":"10.1002/aid2.13397","DOIUrl":null,"url":null,"abstract":"<p>A 63-year-old female presented to our hospital for further management of a rectum lateral spreading lesion discovered by colonoscopy for fecal occult blood survey. Conventional white light colonoscopy showed type 0-IIa + IIb lesion over rectum (Figure 1A). Indigocamine chromoendoscopy showed an irregular mucosal surface pattern (Figure 1B). Subsequent magnifying colonoscopy with narrow-band imaging (NBI) revealed a focal avascular area with scant enlarged, dilated branch-like microvascular pattern on the lesion surface (Figure 1C). 12 MHz endoscopic ultrasound (EUS) showed thickening of mucosal layer (second layer) with preserved muscular propia layer (Figure 1D).</p><p>What is the diagnosis?</p><p>Biopsy specimen showed colon tissue with atypical lymphocytes proliferation above the lamina propria (Figure 2A–E). Immunohistochemical stain showed CK (scant lymphoepithelial lesions), CD138(−), MNDA focal positive, CD20(+), CD79a(+), and PAX-5(+). Mucosa-associated lymphoid tissue lymphoma (MALToma) is diagnosed.</p><p>Primary gastrointestinal non-Hodgkin lymphoma is most often located in the stomach. The large intestine MALToma is rare.<span><sup>1</sup></span> Primary colorectal lymphoma accounts for approximal 10% of gastrointestinal lymphoma and 0.2% of colorectal malignancy.<span><sup>2</sup></span> The gross morphology of colorectal lymphoma could be polyposis, subepithelial tumor, epithelial mass, and ulcerated type under white light endoscopy.<span><sup>3</sup></span> However, flatten type may mimic lateral spreading tumor and be confused with sessile serrated lesion. Image-enhanced colonoscopy was useful for observed microstructure of flatten lesion. Tree-like-appearance blood vessels observed on magnified NBI have been mentioned in colon MALT lymphoma.<span><sup>4</sup></span> In this case, Indogocarmine chromoendoscopy showed irregular mucosal surface pattern, not correlated with EUS finding. NBI magnifying colonoscopy showed Japan NBI Expert Team classification type 3 with branch-like microvascular pattern was the high spot and gave us the hint of colon MALToma.</p><p>The authors declare no conflicts of interest.</p><p>Informed consent was obtained from the patient to publish this article and images.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 2","pages":"107-109"},"PeriodicalIF":0.4000,"publicationDate":"2024-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13397","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13397","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
A 63-year-old female presented to our hospital for further management of a rectum lateral spreading lesion discovered by colonoscopy for fecal occult blood survey. Conventional white light colonoscopy showed type 0-IIa + IIb lesion over rectum (Figure 1A). Indigocamine chromoendoscopy showed an irregular mucosal surface pattern (Figure 1B). Subsequent magnifying colonoscopy with narrow-band imaging (NBI) revealed a focal avascular area with scant enlarged, dilated branch-like microvascular pattern on the lesion surface (Figure 1C). 12 MHz endoscopic ultrasound (EUS) showed thickening of mucosal layer (second layer) with preserved muscular propia layer (Figure 1D).
What is the diagnosis?
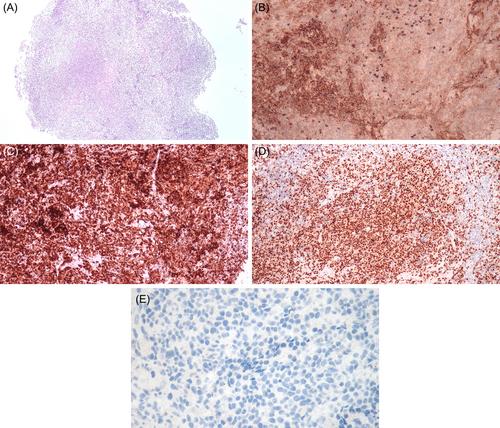
Biopsy specimen showed colon tissue with atypical lymphocytes proliferation above the lamina propria (Figure 2A–E). Immunohistochemical stain showed CK (scant lymphoepithelial lesions), CD138(−), MNDA focal positive, CD20(+), CD79a(+), and PAX-5(+). Mucosa-associated lymphoid tissue lymphoma (MALToma) is diagnosed.
Primary gastrointestinal non-Hodgkin lymphoma is most often located in the stomach. The large intestine MALToma is rare.1 Primary colorectal lymphoma accounts for approximal 10% of gastrointestinal lymphoma and 0.2% of colorectal malignancy.2 The gross morphology of colorectal lymphoma could be polyposis, subepithelial tumor, epithelial mass, and ulcerated type under white light endoscopy.3 However, flatten type may mimic lateral spreading tumor and be confused with sessile serrated lesion. Image-enhanced colonoscopy was useful for observed microstructure of flatten lesion. Tree-like-appearance blood vessels observed on magnified NBI have been mentioned in colon MALT lymphoma.4 In this case, Indogocarmine chromoendoscopy showed irregular mucosal surface pattern, not correlated with EUS finding. NBI magnifying colonoscopy showed Japan NBI Expert Team classification type 3 with branch-like microvascular pattern was the high spot and gave us the hint of colon MALToma.
The authors declare no conflicts of interest.
Informed consent was obtained from the patient to publish this article and images.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


