{"title":"Abdominal pain with radiation to the right thigh in a middle age woman","authors":"Yong-Cheng Ye, Hung-Hsin Lin, Yen-Po Wang","doi":"10.1002/aid2.13396","DOIUrl":null,"url":null,"abstract":"<p>A 43-year-old woman presented with intermittent lower abdominal sharp pain for 4 months, which radiated to her back and right thigh, especially during menstrual period. She denied fever, weight loss, and change in bowel habits, hematochezia, or dysuria. Due to persistent symptoms, colonoscopy was arranged and showed two protruding lesions at the cecum (Figure 1A) and rectosigmoid junction (Figure 1B), respectively. Endoscopic ultrasound (EUS) was arranged for evaluating the originating layer and echogenicity. EUS with miniprobe showed one 25.7 × 9.6 mm heterogeneous hypoechoic mass outside cecum, which was adjacent to the serosa layer (Figure 1C), and one 22.5 × 9.5 mm homogenous hypoechoic mass arising from muscularis propria layer at the rectosigmoid junction (Figure 1D). The differential diagnosis included gastrointestinal stromal tumors, leiomyomas, and schwannomas, which originate from muscularis propria layer and presented as hypoechoic echogenicity.<span><sup>1</sup></span> Symptoms associated with menstrual cycle are an important diagnostic clue for endometriosis, which is detected as hypoechoic lesions on EUS. One 2 × 2 cm cystic lesion in the paracecal area and enlarged appendix were noted during laparoscopy (Figure 2A), and laparoscopic right hemicolectomy was performed due to the will of this patient. Pathological examination is compatible with endometriosis (Figure 2B). Dienogest was used for treatment of rectal endometriosis. The pain improved significantly after surgery and medical therapy.</p><p>Bowel endometriosis accounts for 3.8% to 37% of women with endometriosis and is most commonly involved in rectosigmoid colon, followed by ileocecal region, appendix and other parts of bowel.<span><sup>2</sup></span> Patients with bowel endometriosis may present with dysmenorrhea, infertility or gastrointestinal symptoms. Transvaginal ultrasound is the preferred modality for patients suspected of rectovaginal endometriosis, and EUS can discriminate the depth of infiltration and aids in surgical planning. Bowel endometriotic lesions involve the serosa, muscularis propria, submucosa, and mucosa layer in 94.5%, 95.1%, 37.8% and 6.4% of cases, respectively.<span><sup>3</sup></span></p><p>All authors contribute to all stages of article composition: data acquisition and editing, manuscript drafting, and manuscript revision.</p><p>The authors declare no conflicts of interest.</p><p>The patient authorized the publication of the data and the patient's anonymity is preserved in the article.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 3","pages":"174-176"},"PeriodicalIF":0.4000,"publicationDate":"2024-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13396","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13396","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
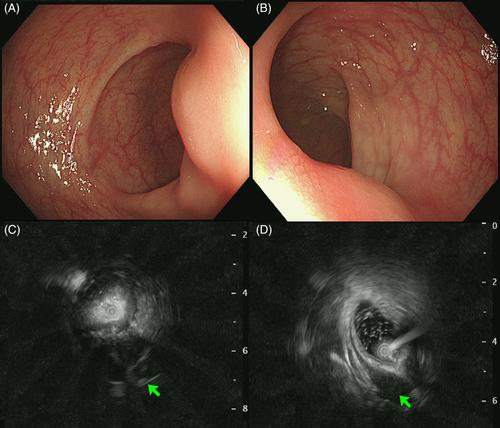
A 43-year-old woman presented with intermittent lower abdominal sharp pain for 4 months, which radiated to her back and right thigh, especially during menstrual period. She denied fever, weight loss, and change in bowel habits, hematochezia, or dysuria. Due to persistent symptoms, colonoscopy was arranged and showed two protruding lesions at the cecum (Figure 1A) and rectosigmoid junction (Figure 1B), respectively. Endoscopic ultrasound (EUS) was arranged for evaluating the originating layer and echogenicity. EUS with miniprobe showed one 25.7 × 9.6 mm heterogeneous hypoechoic mass outside cecum, which was adjacent to the serosa layer (Figure 1C), and one 22.5 × 9.5 mm homogenous hypoechoic mass arising from muscularis propria layer at the rectosigmoid junction (Figure 1D). The differential diagnosis included gastrointestinal stromal tumors, leiomyomas, and schwannomas, which originate from muscularis propria layer and presented as hypoechoic echogenicity.1 Symptoms associated with menstrual cycle are an important diagnostic clue for endometriosis, which is detected as hypoechoic lesions on EUS. One 2 × 2 cm cystic lesion in the paracecal area and enlarged appendix were noted during laparoscopy (Figure 2A), and laparoscopic right hemicolectomy was performed due to the will of this patient. Pathological examination is compatible with endometriosis (Figure 2B). Dienogest was used for treatment of rectal endometriosis. The pain improved significantly after surgery and medical therapy.
Bowel endometriosis accounts for 3.8% to 37% of women with endometriosis and is most commonly involved in rectosigmoid colon, followed by ileocecal region, appendix and other parts of bowel.2 Patients with bowel endometriosis may present with dysmenorrhea, infertility or gastrointestinal symptoms. Transvaginal ultrasound is the preferred modality for patients suspected of rectovaginal endometriosis, and EUS can discriminate the depth of infiltration and aids in surgical planning. Bowel endometriotic lesions involve the serosa, muscularis propria, submucosa, and mucosa layer in 94.5%, 95.1%, 37.8% and 6.4% of cases, respectively.3
All authors contribute to all stages of article composition: data acquisition and editing, manuscript drafting, and manuscript revision.
The authors declare no conflicts of interest.
The patient authorized the publication of the data and the patient's anonymity is preserved in the article.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


