{"title":"Radiation exposure in therapeutic endoscopic retrograde cholangiopancreatography with two types of fluoroscopy systems","authors":"Yao-Sheng Wang, Ying-Jung Wu, Wan-Jou Tseng, Chien-Jui Huang, Chiung-Yu Chen","doi":"10.1002/aid2.13392","DOIUrl":null,"url":null,"abstract":"<p>Fluoroscopy is necessary for endoscopic retrograde cholangiopancreatography (ERCP). Occupational radiation exposure of staff (endoscopists, nurses, or assistants) is inevitable. Fluoroscopes with a tube over-couch (OC) rather than under-couch (UC) may have more radiation reflection dosage on the staff's upper body theoretically, where the most vital organs are. In the study, we assessed the radiation exposure on staff by two different types of fluoroscopes in real-world practice. Using a radiation dosimeter to measure the radiation dosage on endoscopists and assistants in each ERCP procedure under two different fluoroscopic systems (UC vs. OC). Forty-one ERCP procedures were enrolled. Dosimeters were used NanoDots for the measurement of personal radiation exposure. Those dosimeters were attached to the left forearm and chest of the endoscopist and only the chest of two assistants, the wall of the ERCP room, and the controlling room in every procedure. Nine-teen ERCPs were performed under the OC unit, and the other 22 ERCPs were UC method. Fluoroscopic time and output of radiation dose showed no significant difference between the two groups. Radiation exposure in endoscopist were 0.0911[0.1041–0.3974] mGy (OC) versus 0.0276 [0.0080–0.2924] mGy (UC), <i>p</i> < .01 for the forearm; and 0.0318 [0.0070–0.2628] mGy (OC) versus 0.0182 [0.0088–0.1628] mGy (UC), <i>p</i> = .04 for the endoscopist's body. There was no difference in radiation exposure from assistants in both groups. For all the ERCP procedures, the measurement of radiation exposure from high to low is endoscopist's hand, endoscopist's body, assistant 1, assistant 2, and ERCP room (<i>p</i> < .01). Radiation detection from ERCP room is slightly higher but close to controlling room (<i>p</i> = .06). For the safety of occupational radiation protection, tube of fluoroscope UC is better than OC for the endoscopists more than assistants. Besides, the assistant 1 took higher radiation exposure than assistant 2 for each ERCP procedure.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"12 2","pages":""},"PeriodicalIF":0.4000,"publicationDate":"2024-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13392","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13392","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
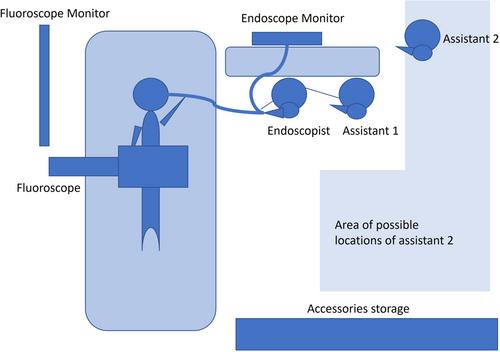
Fluoroscopy is necessary for endoscopic retrograde cholangiopancreatography (ERCP). Occupational radiation exposure of staff (endoscopists, nurses, or assistants) is inevitable. Fluoroscopes with a tube over-couch (OC) rather than under-couch (UC) may have more radiation reflection dosage on the staff's upper body theoretically, where the most vital organs are. In the study, we assessed the radiation exposure on staff by two different types of fluoroscopes in real-world practice. Using a radiation dosimeter to measure the radiation dosage on endoscopists and assistants in each ERCP procedure under two different fluoroscopic systems (UC vs. OC). Forty-one ERCP procedures were enrolled. Dosimeters were used NanoDots for the measurement of personal radiation exposure. Those dosimeters were attached to the left forearm and chest of the endoscopist and only the chest of two assistants, the wall of the ERCP room, and the controlling room in every procedure. Nine-teen ERCPs were performed under the OC unit, and the other 22 ERCPs were UC method. Fluoroscopic time and output of radiation dose showed no significant difference between the two groups. Radiation exposure in endoscopist were 0.0911[0.1041–0.3974] mGy (OC) versus 0.0276 [0.0080–0.2924] mGy (UC), p < .01 for the forearm; and 0.0318 [0.0070–0.2628] mGy (OC) versus 0.0182 [0.0088–0.1628] mGy (UC), p = .04 for the endoscopist's body. There was no difference in radiation exposure from assistants in both groups. For all the ERCP procedures, the measurement of radiation exposure from high to low is endoscopist's hand, endoscopist's body, assistant 1, assistant 2, and ERCP room (p < .01). Radiation detection from ERCP room is slightly higher but close to controlling room (p = .06). For the safety of occupational radiation protection, tube of fluoroscope UC is better than OC for the endoscopists more than assistants. Besides, the assistant 1 took higher radiation exposure than assistant 2 for each ERCP procedure.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


