{"title":"Case of usefulness of drill dilator for pancreatic stone disease in a reverse-Z type main pancreatic duct","authors":"Kenta Yamamoto, Shogo Ota, Toshinao Itani","doi":"10.1111/den.14804","DOIUrl":null,"url":null,"abstract":"<p>Endoscopic pancreatic duct stenting is useful for recurrent chronic obstructive pancreatitis.<span><sup>1, 2</sup></span> However, approaching the caudal pancreatic duct is challenging in patients with severe stenosis or a spiral (loop type) or hairpin (reverse-Z type) curve of the main pancreatic duct.<span><sup>3</sup></span> Recently, a drill dilator (Tornus ES; Olympus, Tokyo, Japan; Fig. 1) has been reported as useful for opening obstructions caused by pancreatic stone impaction.<span><sup>4, 5</sup></span> We encountered a case of pancreatic stone disease in a tortuous main pancreatic duct that was difficult to pass through using conventional devices; a pancreatic stent was successfully implanted using a drill dilator.</p><p>A 68-year-old man with alcoholic chronic pancreatitis was admitted to our hospital with complaints of abdominal pain. Computed tomography showed a large amount of ascites effusion, high amylase level in the ascites, a 7 mm sized pancreatic stone in the main pancreatic duct of the pancreatic head, and caudal pancreatic duct dilatation, suggesting pancreatic duct collapse (Fig. 2a,b). We performed endoscopic retrograde cholangiopancreatography (ERCP), but the device could not pass through because of the reverse-Z type main pancreatic duct and severe stenosis caused by the pancreatic stone (Fig. 2c). The patient improved with conservative treatment alone, but his symptoms flared approximately 6 months later. When we performed ERCP after extracorporeal shock wave lithotripsy for the pancreatic stone disease, the guidewire penetrated the stenosis, but the other devices could not. We used a drill dilator, which easily broke through the stenosis caused by the meandering main pancreatic duct and pancreatic stone (Fig. 2d–f). Afterward, an ERCP cannula (MTW-Endoskopie, Wesel, Germany) could pass through the stenosis, and a pancreatic stent was successfully implanted (Video S1). No adverse events occurred postoperatively.</p><p>The drill dilator, newly designed to advance by rotational manipulation to dilate stenoses, proved valuable by preventing instrument pushing and may inhibit further bend steepening in pancreatic ducts with strong meandering.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":null,"pages":null},"PeriodicalIF":5.0000,"publicationDate":"2024-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14804","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14804","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Endoscopic pancreatic duct stenting is useful for recurrent chronic obstructive pancreatitis.1, 2 However, approaching the caudal pancreatic duct is challenging in patients with severe stenosis or a spiral (loop type) or hairpin (reverse-Z type) curve of the main pancreatic duct.3 Recently, a drill dilator (Tornus ES; Olympus, Tokyo, Japan; Fig. 1) has been reported as useful for opening obstructions caused by pancreatic stone impaction.4, 5 We encountered a case of pancreatic stone disease in a tortuous main pancreatic duct that was difficult to pass through using conventional devices; a pancreatic stent was successfully implanted using a drill dilator.
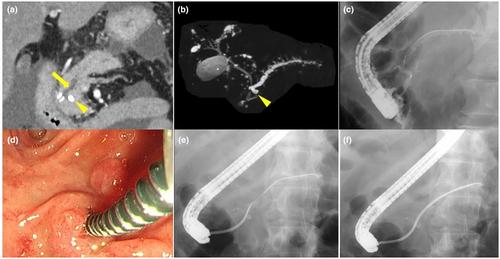
A 68-year-old man with alcoholic chronic pancreatitis was admitted to our hospital with complaints of abdominal pain. Computed tomography showed a large amount of ascites effusion, high amylase level in the ascites, a 7 mm sized pancreatic stone in the main pancreatic duct of the pancreatic head, and caudal pancreatic duct dilatation, suggesting pancreatic duct collapse (Fig. 2a,b). We performed endoscopic retrograde cholangiopancreatography (ERCP), but the device could not pass through because of the reverse-Z type main pancreatic duct and severe stenosis caused by the pancreatic stone (Fig. 2c). The patient improved with conservative treatment alone, but his symptoms flared approximately 6 months later. When we performed ERCP after extracorporeal shock wave lithotripsy for the pancreatic stone disease, the guidewire penetrated the stenosis, but the other devices could not. We used a drill dilator, which easily broke through the stenosis caused by the meandering main pancreatic duct and pancreatic stone (Fig. 2d–f). Afterward, an ERCP cannula (MTW-Endoskopie, Wesel, Germany) could pass through the stenosis, and a pancreatic stent was successfully implanted (Video S1). No adverse events occurred postoperatively.
The drill dilator, newly designed to advance by rotational manipulation to dilate stenoses, proved valuable by preventing instrument pushing and may inhibit further bend steepening in pancreatic ducts with strong meandering.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


