Jeffrey Dalli, Jonathan P. Epperlein, Niall P. Hardy, Mohammad Faraz Khan, Pol Mac Aonghusa, Ronan A. Cahill
{"title":"Clinical and computational development of a patient-calibrated ICGFA bowel transection recommender","authors":"Jeffrey Dalli, Jonathan P. Epperlein, Niall P. Hardy, Mohammad Faraz Khan, Pol Mac Aonghusa, Ronan A. Cahill","doi":"10.1007/s00464-024-10827-6","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>Intraoperative indocyanine green fluorescence angiography (ICGFA) aims to reduce colorectal anastomotic complications. However, signal interpretation is inconsistent and confounded by patient physiology and system behaviours. Here, we demonstrate a proof of concept of a novel clinical and computational method for patient calibrated quantitative ICGFA (QICGFA) bowel transection recommendation.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>Patients undergoing elective colorectal resection had colonic ICGFA both immediately after operative commencement prior to any dissection and again, as usual, just before anastomotic construction. Video recordings of both ICGFA acquisitions were blindly quantified post hoc across selected colonic regions of interest (ROIs) using tracking-quantification software and computationally compared with satisfactory perfusion assumed in second time-point ROIs, demonstrating 85% agreement with baseline ICGFA. ROI quantification outputs detailing projected perfusion sufficiency-insufficiency zones were compared to the actual surgeon-selected transection/anastomotic construction site for left/right-sided resections, respectively. Anastomotic outcomes were recorded, and tissue lactate was also measured in the devascularised colonic segment in a subgroup of patients. The novel perfusion zone projections were developed as full-screen recommendations via overlay heatmaps.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>No patient suffered intra- or early postoperative anastomotic complications. Following computational development (<i>n</i> = 14) the software recommended zone (ROI) contained the expert surgical site of transection in almost all cases (Jaccard similarity index 0.91) of the nine patient validation series. Previously published ICGFA time-series milestone descriptors correlated moderately well, but lactate measurements did not. High resolution augmented reality heatmaps presenting recommendations from all pixels of the bowel ICGFA were generated for all cases.</p><h3 data-test=\"abstract-sub-heading\">Conclusions</h3><p>By benchmarking to the patient’s own baseline perfusion, this novel QICGFA method could allow the deployment of algorithmic personalised NIR bowel transection point recommendation in a way fitting existing clinical workflow.</p>","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"154 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-10827-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Intraoperative indocyanine green fluorescence angiography (ICGFA) aims to reduce colorectal anastomotic complications. However, signal interpretation is inconsistent and confounded by patient physiology and system behaviours. Here, we demonstrate a proof of concept of a novel clinical and computational method for patient calibrated quantitative ICGFA (QICGFA) bowel transection recommendation.
Methods
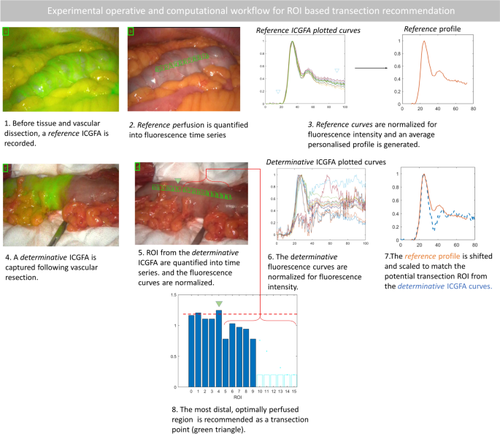
Patients undergoing elective colorectal resection had colonic ICGFA both immediately after operative commencement prior to any dissection and again, as usual, just before anastomotic construction. Video recordings of both ICGFA acquisitions were blindly quantified post hoc across selected colonic regions of interest (ROIs) using tracking-quantification software and computationally compared with satisfactory perfusion assumed in second time-point ROIs, demonstrating 85% agreement with baseline ICGFA. ROI quantification outputs detailing projected perfusion sufficiency-insufficiency zones were compared to the actual surgeon-selected transection/anastomotic construction site for left/right-sided resections, respectively. Anastomotic outcomes were recorded, and tissue lactate was also measured in the devascularised colonic segment in a subgroup of patients. The novel perfusion zone projections were developed as full-screen recommendations via overlay heatmaps.
Results
No patient suffered intra- or early postoperative anastomotic complications. Following computational development (n = 14) the software recommended zone (ROI) contained the expert surgical site of transection in almost all cases (Jaccard similarity index 0.91) of the nine patient validation series. Previously published ICGFA time-series milestone descriptors correlated moderately well, but lactate measurements did not. High resolution augmented reality heatmaps presenting recommendations from all pixels of the bowel ICGFA were generated for all cases.
Conclusions
By benchmarking to the patient’s own baseline perfusion, this novel QICGFA method could allow the deployment of algorithmic personalised NIR bowel transection point recommendation in a way fitting existing clinical workflow.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


