Pan Pan, Yue Wang, Chang Liu, Yanhui Tu, Haibo Cheng, Qingyun Yang, Fei Xie, Yuan Li, Lixin Xie, Yuhong Liu
{"title":"Revisiting the potential value of vital signs in the real-time prediction of mortality risk in intensive care unit patients","authors":"Pan Pan, Yue Wang, Chang Liu, Yanhui Tu, Haibo Cheng, Qingyun Yang, Fei Xie, Yuan Li, Lixin Xie, Yuhong Liu","doi":"10.1186/s40537-024-00896-8","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Predicting patient mortality risk facilitates early intervention in intensive care unit (ICU) patients at greater risk of disease progression. This study applies machine learning methods to multidimensional clinical data to dynamically predict mortality risk in ICU patients.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>A total of 33,798 patients in the MIMIC-III database were collected. An integrated model NIMRF (Network Integrating Memory Module and Random Forest) based on multidimensional variables such as vital sign variables and laboratory variables was developed to predict the risk of death for ICU patients in four non overlapping time windows of 0–1 h, 1–3 h, 3–6 h, and 6–12 h. Mortality risk in four nonoverlapping time windows of 12 h was externally validated on data from 889 patients in the respiratory critical care unit of the Chinese PLA General Hospital and compared with LSTM, random forest and time-dependent cox regression model (survival analysis) methods. We also interpret the developed model to obtain important factors for predicting mortality risk across time windows. The code can be found in https://github.com/wyuexiao/NIMRF.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>The NIMRF model developed in this study could predict the risk of death in four nonoverlapping time windows (0–1 h, 1–3 h, 3–6 h, 6–12 h) after any time point in ICU patients, and in internal data validation, it is suggested that the model is more accurate than LSTM, random forest prediction and time-dependent cox regression model (area under receiver operating characteristic curve, or AUC, 0–1 h: 0.8015 [95% CI 0.7725–0.8304] vs. 0.7144 [95%] CI 0.6824–0.7464] vs. 0.7606 [95% CI 0.7300–0.7913] vs 0.3867 [95% CI 0.3573–0.4161]; 1–3 h: 0.7100 [95% CI 0.6777–0.7423] vs. 0.6389 [95% CI 0.6055–0.6723] vs. 0.6992 [95% CI 0.6667–0.7318] vs 0.3854 [95% CI 0.3559–0.4150]; 3–6 h: 0.6760 [95% CI 0.6425–0.7097] vs. 0.5964 [95% CI 0.5622–0.6306] vs. 0.6760 [95% CI 0.6427–0.7099] vs 0.3967 [95% CI 0.3662–0.4271]; 6–12 h: 0.6380 [0.6031–0.6729] vs. 0.6032 [0.5705–0.6406] vs. 0.6055 [0.5682–0.6383] vs 0.4023 [95% CI 0.3709–0.4337]). External validation was performed on the data of patients in the respiratory critical care unit of the Chinese PLA General Hospital. Compared with LSTM, random forest and time-dependent cox regression model, the NIMRF model was still the best, with an AUC of 0.9366 [95% CI 0.9157–0.9575 for predicting death risk in 0–1 h]. The corresponding AUCs of LSTM, random forest and time-dependent cox regression model were 0.9263 [95% CI 0.9039–0.9486], 0.7437 [95% CI 0.7083–0.7791] and 0.2447 [95% CI 0.2202–0.2692], respectively. Interpretation of the model revealed that vital signs (systolic blood pressure, heart rate, diastolic blood pressure, respiratory rate, and body temperature) were highly correlated with events of death.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Using the NIMRF model can integrate ICU multidimensional variable data, especially vital sign variable data, to accurately predict the death events of ICU patients. These predictions can assist clinicians in choosing more timely and precise treatment methods and interventions and, more importantly, can reduce invasive procedures and save medical costs.</p>","PeriodicalId":15158,"journal":{"name":"Journal of Big Data","volume":"11 1","pages":""},"PeriodicalIF":6.4000,"publicationDate":"2024-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Big Data","FirstCategoryId":"94","ListUrlMain":"https://doi.org/10.1186/s40537-024-00896-8","RegionNum":2,"RegionCategory":"计算机科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"COMPUTER SCIENCE, THEORY & METHODS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Predicting patient mortality risk facilitates early intervention in intensive care unit (ICU) patients at greater risk of disease progression. This study applies machine learning methods to multidimensional clinical data to dynamically predict mortality risk in ICU patients.
Methods
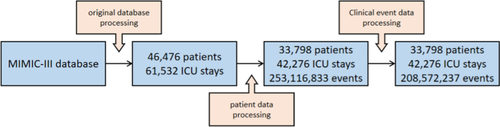
A total of 33,798 patients in the MIMIC-III database were collected. An integrated model NIMRF (Network Integrating Memory Module and Random Forest) based on multidimensional variables such as vital sign variables and laboratory variables was developed to predict the risk of death for ICU patients in four non overlapping time windows of 0–1 h, 1–3 h, 3–6 h, and 6–12 h. Mortality risk in four nonoverlapping time windows of 12 h was externally validated on data from 889 patients in the respiratory critical care unit of the Chinese PLA General Hospital and compared with LSTM, random forest and time-dependent cox regression model (survival analysis) methods. We also interpret the developed model to obtain important factors for predicting mortality risk across time windows. The code can be found in https://github.com/wyuexiao/NIMRF.
Results
The NIMRF model developed in this study could predict the risk of death in four nonoverlapping time windows (0–1 h, 1–3 h, 3–6 h, 6–12 h) after any time point in ICU patients, and in internal data validation, it is suggested that the model is more accurate than LSTM, random forest prediction and time-dependent cox regression model (area under receiver operating characteristic curve, or AUC, 0–1 h: 0.8015 [95% CI 0.7725–0.8304] vs. 0.7144 [95%] CI 0.6824–0.7464] vs. 0.7606 [95% CI 0.7300–0.7913] vs 0.3867 [95% CI 0.3573–0.4161]; 1–3 h: 0.7100 [95% CI 0.6777–0.7423] vs. 0.6389 [95% CI 0.6055–0.6723] vs. 0.6992 [95% CI 0.6667–0.7318] vs 0.3854 [95% CI 0.3559–0.4150]; 3–6 h: 0.6760 [95% CI 0.6425–0.7097] vs. 0.5964 [95% CI 0.5622–0.6306] vs. 0.6760 [95% CI 0.6427–0.7099] vs 0.3967 [95% CI 0.3662–0.4271]; 6–12 h: 0.6380 [0.6031–0.6729] vs. 0.6032 [0.5705–0.6406] vs. 0.6055 [0.5682–0.6383] vs 0.4023 [95% CI 0.3709–0.4337]). External validation was performed on the data of patients in the respiratory critical care unit of the Chinese PLA General Hospital. Compared with LSTM, random forest and time-dependent cox regression model, the NIMRF model was still the best, with an AUC of 0.9366 [95% CI 0.9157–0.9575 for predicting death risk in 0–1 h]. The corresponding AUCs of LSTM, random forest and time-dependent cox regression model were 0.9263 [95% CI 0.9039–0.9486], 0.7437 [95% CI 0.7083–0.7791] and 0.2447 [95% CI 0.2202–0.2692], respectively. Interpretation of the model revealed that vital signs (systolic blood pressure, heart rate, diastolic blood pressure, respiratory rate, and body temperature) were highly correlated with events of death.
Conclusion
Using the NIMRF model can integrate ICU multidimensional variable data, especially vital sign variable data, to accurately predict the death events of ICU patients. These predictions can assist clinicians in choosing more timely and precise treatment methods and interventions and, more importantly, can reduce invasive procedures and save medical costs.
背景预测患者的死亡风险有助于对疾病进展风险较大的重症监护室(ICU)患者进行早期干预。本研究将机器学习方法应用于多维临床数据,以动态预测重症监护病房患者的死亡风险。基于生命体征变量和实验室变量等多维变量,建立了一个集成模型NIMRF(网络集成记忆模块和随机森林),用于预测ICU患者在0-1小时、1-3小时、3-6小时和6-12小时四个非重叠时间窗内的死亡风险。在中国人民解放军总医院呼吸重症监护室 889 名患者的数据中对 12 小时内四个非重叠时间窗的死亡风险进行了外部验证,并与 LSTM、随机森林和时间依赖性 cox 回归模型(生存分析)方法进行了比较。我们还对所开发的模型进行了解释,以获得预测跨时间窗死亡风险的重要因素。本研究开发的 NIMRF 模型可预测 ICU 患者任意时间点后四个非重叠时间窗(0-1 h、1-3 h、3-6 h、6-12 h)内的死亡风险,内部数据验证表明,该模型比 LSTM、随机森林预测和时间依赖性 cox 回归模型更准确(接收器操作特征曲线下面积,或 AUC,0-1 h:0.8015 [95% CI 0.7725-0.8304] vs. 0.7144 [95%] CI 0.6824-0.7464] vs. 0.7606 [95% CI 0.7300-0.7913] vs. 0.3867 [95% CI 0.3573-0.4161]; 1-3 h: 0.7100 [95% CI 0.6777-0.7423] vs. 0.6389 [95% CI 0.6055-0.6723] vs. 0.6992 [95% CI 0.6667-0.7318] vs. 0.3854 [95% CI 0.3559-0.4150]; 3-6 h:0.6760 [95% CI 0.6425-0.7097] vs. 0.5964 [95% CI 0.5622-0.6306] vs. 0.6760 [95% CI 0.6427-0.7099] vs. 0.3967 [95% CI 0.3662-0.6-12小时:0.6380 [0.6031-0.6729] vs. 0.6032 [0.5705-0.6406] vs. 0.6055 [0.5682-0.6383] vs. 0.4023 [95% CI 0.3709-0.4337])。外部验证在中国人民解放军总医院呼吸重症监护室的患者数据中进行。与 LSTM、随机森林和时间依赖性 cox 回归模型相比,NIMRF 模型的 AUC 为 0.9366 [95% CI 0.9157-0.9575(预测 0-1 h 死亡风险)],仍然是最好的。LSTM、随机森林和时间依赖性 cox 回归模型的相应 AUC 分别为 0.9263 [95% CI 0.9039-0.9486]、0.7437 [95% CI 0.7083-0.7791]和 0.2447 [95% CI 0.2202-0.2692]。结论使用 NIMRF 模型可以整合 ICU 多维变量数据,尤其是生命体征变量数据,从而准确预测 ICU 患者的死亡事件。这些预测可以帮助临床医生选择更及时、更精确的治疗方法和干预措施,更重要的是,可以减少侵入性程序,节约医疗成本。
期刊介绍:
The Journal of Big Data publishes high-quality, scholarly research papers, methodologies, and case studies covering a broad spectrum of topics, from big data analytics to data-intensive computing and all applications of big data research. It addresses challenges facing big data today and in the future, including data capture and storage, search, sharing, analytics, technologies, visualization, architectures, data mining, machine learning, cloud computing, distributed systems, and scalable storage. The journal serves as a seminal source of innovative material for academic researchers and practitioners alike.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


