D. J. Nijssen, J. J. Joosten, J. Osterkamp, R. M. van den Elzen, D. M. de Bruin, M. B. S. Svendsen, M. W. Dalsgaard, S. S. Gisbertz, R. Hompes, M. P. Achiam, M. I. van Berge Henegouwen
{"title":"Quantification of fluorescence angiography for visceral perfusion assessment: measuring agreement between two software algorithms","authors":"D. J. Nijssen, J. J. Joosten, J. Osterkamp, R. M. van den Elzen, D. M. de Bruin, M. B. S. Svendsen, M. W. Dalsgaard, S. S. Gisbertz, R. Hompes, M. P. Achiam, M. I. van Berge Henegouwen","doi":"10.1007/s00464-024-10794-y","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Indocyanine green fluorescence angiography (ICG-FA) may reduce perfusion-related complications of gastrointestinal anastomosis. Software implementations for quantifying ICG-FA are emerging to overcome a subjective interpretation of the technology. Comparison between quantification algorithms is needed to judge its external validity. This study aimed to measure the agreement for visceral perfusion assessment between two independently developed quantification software implementations.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>This retrospective cohort analysis included standardized ICG-FA video recordings of patients who underwent esophagectomy with gastric conduit reconstruction between August 2020 until February 2022. Recordings were analyzed by two quantification software implementations: AMS and CPH. The quantitative parameter used to measure visceral perfusion was the <i>normalized maximum slope</i> derived from fluorescence time curves. The agreement between AMS and CPH was evaluated in a Bland–Altman analysis. The relation between the intraoperative measurement of perfusion and the incidence of anastomotic leakage was determined for both software implementations.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Seventy pre-anastomosis ICG-FA recordings were included in the study. The Bland–Altman analysis indicated a mean relative difference of + 58.2% in the measurement of the <i>normalized maximum slope</i> when comparing the AMS software to CPH. The agreement between AMS and CPH deteriorated as the magnitude of the measured values increased, revealing a proportional (linear) bias (<i>R</i><sup>2</sup> = 0.512, <i>p</i> < 0.001). Neither the AMS nor the CPH measurements of the <i>normalized maximum slope</i> held a significant relationship with the occurrence of anastomotic leakage (median of 0.081 versus 0.074, <i>p</i> = 0.32 and 0.041 vs 0.042, <i>p</i> = 0.51, respectively).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>This is the first study to demonstrate technical differences in software implementations that can lead to discrepancies in ICG-FA quantification in human clinical cases. The possible variation among software-based quantification methods should be considered when interpreting studies that report quantitative ICG-FA parameters and derived thresholds, as there may be a limited external validity.</p>","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"298 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-10794-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Indocyanine green fluorescence angiography (ICG-FA) may reduce perfusion-related complications of gastrointestinal anastomosis. Software implementations for quantifying ICG-FA are emerging to overcome a subjective interpretation of the technology. Comparison between quantification algorithms is needed to judge its external validity. This study aimed to measure the agreement for visceral perfusion assessment between two independently developed quantification software implementations.
Methods
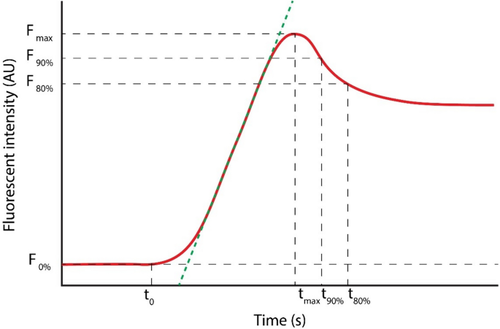
This retrospective cohort analysis included standardized ICG-FA video recordings of patients who underwent esophagectomy with gastric conduit reconstruction between August 2020 until February 2022. Recordings were analyzed by two quantification software implementations: AMS and CPH. The quantitative parameter used to measure visceral perfusion was the normalized maximum slope derived from fluorescence time curves. The agreement between AMS and CPH was evaluated in a Bland–Altman analysis. The relation between the intraoperative measurement of perfusion and the incidence of anastomotic leakage was determined for both software implementations.
Results
Seventy pre-anastomosis ICG-FA recordings were included in the study. The Bland–Altman analysis indicated a mean relative difference of + 58.2% in the measurement of the normalized maximum slope when comparing the AMS software to CPH. The agreement between AMS and CPH deteriorated as the magnitude of the measured values increased, revealing a proportional (linear) bias (R2 = 0.512, p < 0.001). Neither the AMS nor the CPH measurements of the normalized maximum slope held a significant relationship with the occurrence of anastomotic leakage (median of 0.081 versus 0.074, p = 0.32 and 0.041 vs 0.042, p = 0.51, respectively).
Conclusion
This is the first study to demonstrate technical differences in software implementations that can lead to discrepancies in ICG-FA quantification in human clinical cases. The possible variation among software-based quantification methods should be considered when interpreting studies that report quantitative ICG-FA parameters and derived thresholds, as there may be a limited external validity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


